Anda mungkin juga menyukai
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Hypoxia-Modified Cancer Cell MetabolismDokumen15 halamanHypoxia-Modified Cancer Cell Metabolismdana ursuBelum ada peringkat
- Pharmaceutical Sciences: Targeting Hif-1 Pathway: A Therapeutic Approach To Kill Cancer CellsDokumen6 halamanPharmaceutical Sciences: Targeting Hif-1 Pathway: A Therapeutic Approach To Kill Cancer CellsBaru Chandrasekhar RaoBelum ada peringkat
- Hypoxia Paper PDFDokumen11 halamanHypoxia Paper PDFMogaime BuendiaBelum ada peringkat
- Nitric Oxide NEWDokumen71 halamanNitric Oxide NEWP meruguBelum ada peringkat
- Komparasi Inergen, FM-200, Dan Novec 1230Dokumen4 halamanKomparasi Inergen, FM-200, Dan Novec 1230Bagus PrambudiBelum ada peringkat
- Blast Injury ManagementDokumen16 halamanBlast Injury Managementheart wisdomBelum ada peringkat
- Performance of Three Large-Volume Infusion Pumps With The Monoplace Hyperbaric ChamberDokumen11 halamanPerformance of Three Large-Volume Infusion Pumps With The Monoplace Hyperbaric Chambertonylee24Belum ada peringkat
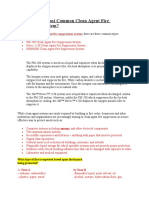
- TYPES OF Clean Agent Fire Suppression SystemDokumen4 halamanTYPES OF Clean Agent Fire Suppression SystemRaju GBelum ada peringkat
- Hyperbaric EnvironmentDokumen20 halamanHyperbaric Environmentdeepuphysio100% (2)
- Oxygen Therapy IMA 2018-1Dokumen49 halamanOxygen Therapy IMA 2018-1Tarsisius Ryang TobyBelum ada peringkat
- The Circulation: Blood Pressure RegulationDokumen42 halamanThe Circulation: Blood Pressure RegulationLouis JinBelum ada peringkat
- Riding The WavesDokumen76 halamanRiding The WavesMedic03431Belum ada peringkat
- Role of Hypoxia in Cancer Therapy by Regulating The Tumor MicroenvironmentDokumen15 halamanRole of Hypoxia in Cancer Therapy by Regulating The Tumor MicroenvironmentShuang LiBelum ada peringkat
- Hyperbaric Facilities Maintenance Manual: Navfac Mo-406 JULY 1990Dokumen184 halamanHyperbaric Facilities Maintenance Manual: Navfac Mo-406 JULY 1990stalin_83Belum ada peringkat
- Transport of Respiratory GasesDokumen27 halamanTransport of Respiratory GasesSyahmi Ieskandar100% (1)
- Baska MaskDokumen8 halamanBaska MaskAnish H DaveBelum ada peringkat
- StrokeDokumen102 halamanStrokea20-0353-958Belum ada peringkat
- Oxygen CascadeDokumen12 halamanOxygen Cascadehy3pjb1984Belum ada peringkat
- Respiratory DrugsDokumen20 halamanRespiratory DrugsMelanesiaBelum ada peringkat
- Bronchial AsthmaDokumen25 halamanBronchial AsthmaKamil HannaBelum ada peringkat
- Spiro Me Try Cheat Sheet 09Dokumen2 halamanSpiro Me Try Cheat Sheet 09Yudha Perwira PutraBelum ada peringkat
- Toxicology Case Studies Carbon MonoxideDokumen5 halamanToxicology Case Studies Carbon MonoxideMark Jayson T. AsinoBelum ada peringkat
- 2022 Book Wireless Mobile Communication andDokumen365 halaman2022 Book Wireless Mobile Communication andPhan Thanh DoBelum ada peringkat
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDokumen25 halamanSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13Belum ada peringkat
- Riding The Waves Handout R6Dokumen35 halamanRiding The Waves Handout R6Darryl Betts100% (2)
- C H P O: Andidate Andbook Rogram UtlineDokumen9 halamanC H P O: Andidate Andbook Rogram UtlineSuryadinata MomingBelum ada peringkat
- Chapter 4Dokumen24 halamanChapter 4Sulaiman Al-qarawnehBelum ada peringkat
- Capnography Reference Handbook: Capnostat Loflo Flotrak Elite AccessoriesDokumen40 halamanCapnography Reference Handbook: Capnostat Loflo Flotrak Elite AccessoriesLizzie RamosBelum ada peringkat
- AFL Record - Hyperbaric ChamberDokumen2 halamanAFL Record - Hyperbaric ChamberDocRichoBelum ada peringkat
- A Powerful Tool To Objectively Monitor Your Patients Ventilatory StatusDokumen36 halamanA Powerful Tool To Objectively Monitor Your Patients Ventilatory StatusBeth Strom-Sturm100% (1)
- Therapeutic Effects of Hyperbaric Oxygen IntegratedDokumen4 halamanTherapeutic Effects of Hyperbaric Oxygen IntegratedWilson Castro O.Belum ada peringkat
- 10 AsthmaDokumen39 halaman10 AsthmaAkash MishraBelum ada peringkat
- Isbi Practice Guidelines For Burn Care Part 2 2018 PDFDokumen90 halamanIsbi Practice Guidelines For Burn Care Part 2 2018 PDFAstri SuyataBelum ada peringkat
- Adams ValveDokumen5 halamanAdams ValveSuresh KumarBelum ada peringkat
- A Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical CasesDokumen5 halamanA Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical Casesnethra nitinBelum ada peringkat
- Perioperative AnaphylaxisDokumen23 halamanPerioperative AnaphylaxiscrackernetBelum ada peringkat
- WCHM-Winter-2017 12 28 PDFDokumen39 halamanWCHM-Winter-2017 12 28 PDFNiekeBelum ada peringkat
- Hyerbaric Oxygenation - Final DraftDokumen17 halamanHyerbaric Oxygenation - Final Draftapi-542958465Belum ada peringkat
- Anaesthesia For LapDokumen91 halamanAnaesthesia For LapAbhyuday KumarBelum ada peringkat
- Deep Sea Diving Physiology - Lecture by DR Syma RizanDokumen35 halamanDeep Sea Diving Physiology - Lecture by DR Syma RizanLapyasonta NaradiargaBelum ada peringkat
- Oxygen Therapy and Administration V2Dokumen32 halamanOxygen Therapy and Administration V2SteffiBelum ada peringkat
- Biomedical New Hire OrientationDokumen29 halamanBiomedical New Hire OrientationBEJOYBelum ada peringkat
- Racial Bias in Pulse Oximetry Measurement: CorrespondenceDokumen2 halamanRacial Bias in Pulse Oximetry Measurement: CorrespondenceYony Gutierrez100% (1)
- Aeroneb Solo DFU - EN - Rev JDokumen56 halamanAeroneb Solo DFU - EN - Rev Jyagnaashi9092Belum ada peringkat
- Pulmonary SystemDokumen75 halamanPulmonary Systemangeles_robert_71Belum ada peringkat
- 14 NSAIDS LastDokumen46 halaman14 NSAIDS LastMewael TesfamichaelBelum ada peringkat
- Fluid ResuscitationDokumen3 halamanFluid ResuscitationAdam FnsBelum ada peringkat
- Analgesics: L. SchefflerDokumen32 halamanAnalgesics: L. SchefflerNovita_PemalangBelum ada peringkat
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDokumen8 halamanBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamBelum ada peringkat
- Hyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMODokumen63 halamanHyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMOAkbar AmirullahBelum ada peringkat
- Airway Skills 2 - Bag Valve MaskDokumen4 halamanAirway Skills 2 - Bag Valve MaskRinna MauLiddaBelum ada peringkat
- Infant Incubator: Faqih Auliya Muhammad (P23138116014) Hotmatua Lubis (P23138116021)Dokumen18 halamanInfant Incubator: Faqih Auliya Muhammad (P23138116014) Hotmatua Lubis (P23138116021)Faqih AuliyaBelum ada peringkat
- Advanced Airway Management 4th YearsDokumen39 halamanAdvanced Airway Management 4th YearsAmmaarah Isaacs100% (1)
- History of FluorosDokumen2 halamanHistory of FluorosEvi DianBelum ada peringkat
- ImmunotoxicityDokumen6 halamanImmunotoxicitysuba_n23100% (1)
- Hypoxia and CyanosisDokumen33 halamanHypoxia and CyanosisRamlah IbrahimBelum ada peringkat
- Measuring Pulse OximeterDokumen94 halamanMeasuring Pulse OximeterMuhammed HammadBelum ada peringkat
- Update On The Management of Upper Gastrointestinal BleedingDokumen12 halamanUpdate On The Management of Upper Gastrointestinal Bleedingakbar011512Belum ada peringkat
- Clinical Study: A Role For Postoperative Negative Pressure Wound Therapy in Multitissue Hand InjuriesDokumen8 halamanClinical Study: A Role For Postoperative Negative Pressure Wound Therapy in Multitissue Hand InjuriesAmriansyah PranowoBelum ada peringkat
- Lesson 3 - Practical ResearchDokumen17 halamanLesson 3 - Practical ResearchBenBelum ada peringkat
- Lazard Levelized Cost of Storage v20Dokumen46 halamanLazard Levelized Cost of Storage v20macBelum ada peringkat
- Freeman Has Been A Partner in A Commercial Construction CompanyDokumen1 halamanFreeman Has Been A Partner in A Commercial Construction CompanyMuhammad ShahidBelum ada peringkat
- Culture-Partners M&A EbookDokumen12 halamanCulture-Partners M&A EbookapachemonoBelum ada peringkat
- Linear Analysis of Concrete Frames Considering Joint FlexibilityDokumen16 halamanLinear Analysis of Concrete Frames Considering Joint FlexibilityluffiM13Belum ada peringkat
- A-Health Advance - Application Form With InstructionsDokumen14 halamanA-Health Advance - Application Form With InstructionsExsan OthmanBelum ada peringkat
- AYURVEDA Products CatalogDokumen17 halamanAYURVEDA Products CatalogFoutanke TorodoBelum ada peringkat
- Analog Digital Thermopile Application Note PDFDokumen18 halamanAnalog Digital Thermopile Application Note PDFGopal HegdeBelum ada peringkat
- Radiology PearlsDokumen2 halamanRadiology PearlsSalman Rashid100% (2)
- Pipe Support Reference 8-29-14Dokumen108 halamanPipe Support Reference 8-29-14HITESHBelum ada peringkat
- Forms of Organizing Activity Games, Methodology of Conducting Activity Games in Physical Education LessonsDokumen4 halamanForms of Organizing Activity Games, Methodology of Conducting Activity Games in Physical Education LessonsAcademic JournalBelum ada peringkat
- FM Assignment 17-M-518 MMM - Eicher MotorDokumen33 halamanFM Assignment 17-M-518 MMM - Eicher MotorTrilokBelum ada peringkat
- Raw:/storage/emulated/0/download/1623980378472 - 1623980347729 - PE 4 Module 2Dokumen11 halamanRaw:/storage/emulated/0/download/1623980378472 - 1623980347729 - PE 4 Module 2Marvin Espenocilla EspeñoBelum ada peringkat
- Ce-424 PM&CDokumen11 halamanCe-424 PM&CAaqib ShoukatBelum ada peringkat
- Fall 2015 The Language of Anatomy PDFDokumen14 halamanFall 2015 The Language of Anatomy PDFpikminixBelum ada peringkat
- MATLAB PROGRAMMING An Engineering PerspectiveDokumen129 halamanMATLAB PROGRAMMING An Engineering PerspectivelolaBelum ada peringkat
- Downloaded From Manuals Search EngineDokumen14 halamanDownloaded From Manuals Search EngineAl AlBelum ada peringkat
- Punctuation WorksheetsDokumen10 halamanPunctuation WorksheetsRehan Sadiq100% (2)
- Attention: 6R60/6R75/6R80 Installation GuideDokumen4 halamanAttention: 6R60/6R75/6R80 Installation GuideEdwinferBelum ada peringkat
- Hex 33 X 80Dokumen1 halamanHex 33 X 80PurchaseBelum ada peringkat
- Irregular Verbs Lesson PlanDokumen13 halamanIrregular Verbs Lesson Planapi-311868026Belum ada peringkat
- Assessment of Locomotive and Multi-Unit Fatigue Strength Considering The Results of Certifi Cation Tests in Ukraine and EU CountriesDokumen8 halamanAssessment of Locomotive and Multi-Unit Fatigue Strength Considering The Results of Certifi Cation Tests in Ukraine and EU CountriesLeonardo Antônio Pereira100% (1)
- Amended August 8 2016Dokumen31 halamanAmended August 8 2016lux186Belum ada peringkat
- 7TH Maths F.a-1Dokumen1 halaman7TH Maths F.a-1Marrivada SuryanarayanaBelum ada peringkat
- Manual G Ingles - V6Dokumen68 halamanManual G Ingles - V6Phùng Thế Kiên50% (2)
- Performance Task 1st Quarter Poetry Writing WorkshopDokumen3 halamanPerformance Task 1st Quarter Poetry Writing WorkshopNicole john ZuluetaBelum ada peringkat
- CV (Martin A Johnson)Dokumen7 halamanCV (Martin A Johnson)kganesanBelum ada peringkat
- Modal Verbs EjercicioDokumen2 halamanModal Verbs EjercicioAngel sosaBelum ada peringkat
- Foundstone Hacme Bank User and Solution Guide v2.0Dokumen60 halamanFoundstone Hacme Bank User and Solution Guide v2.0Yeison MorenoBelum ada peringkat
- Lesson Plan 2 BasketballDokumen3 halamanLesson Plan 2 Basketballapi-313716520100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (33)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDari EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDPenilaian: 5 dari 5 bintang5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 4.5 dari 5 bintang4.5/5 (82)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Dari EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Penilaian: 3 dari 5 bintang3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceDari EverandTo Explain the World: The Discovery of Modern SciencePenilaian: 3.5 dari 5 bintang3.5/5 (51)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePenilaian: 2 dari 5 bintang2/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 4 dari 5 bintang4/5 (4)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeDari EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgePenilaian: 4.5 dari 5 bintang4.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDari EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDari EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesPenilaian: 4.5 dari 5 bintang4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsPenilaian: 5 dari 5 bintang5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDari EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsPenilaian: 4.5 dari 5 bintang4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDari EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifePenilaian: 4.5 dari 5 bintang4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDari EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryPenilaian: 4 dari 5 bintang4/5 (46)
- The Marshmallow Test: Mastering Self-ControlDari EverandThe Marshmallow Test: Mastering Self-ControlPenilaian: 4.5 dari 5 bintang4.5/5 (60)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDari EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsBelum ada peringkat
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIDari EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIPenilaian: 4 dari 5 bintang4/5 (20)