Anda mungkin juga menyukai
- CFLGA Handbook - Section On Assessment CriteriaDokumen25 halamanCFLGA Handbook - Section On Assessment CriteriaJim100% (6)
- Admission and Discharge Record: Doc Jo - An Lying - in ClinicDokumen25 halamanAdmission and Discharge Record: Doc Jo - An Lying - in ClinicJo-An Marie Aguedan100% (1)
- Prenatal CardDokumen2 halamanPrenatal CardMandeep SinghBelum ada peringkat
- Form 4. TX Ipt Card v061416Dokumen2 halamanForm 4. TX Ipt Card v061416Emmanuel GorresBelum ada peringkat
- Dianne A. Evangelista, M.D: Measuring and Learning Together Towards ResultsDokumen59 halamanDianne A. Evangelista, M.D: Measuring and Learning Together Towards ResultsKath DellosaBelum ada peringkat
- Health Screening and Assessment Form - SampleDokumen3 halamanHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- History and Physical ExaminationDokumen4 halamanHistory and Physical ExaminationVernonDimalBelum ada peringkat
- History Taking FormDokumen14 halamanHistory Taking FormFebbie ArcalesBelum ada peringkat
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Dokumen6 halamanAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruBelum ada peringkat
- Obstetric FormDokumen4 halamanObstetric FormKhylamarie VillalunaBelum ada peringkat
- Med HX and PE Wards FormDokumen8 halamanMed HX and PE Wards FormFMDCBelum ada peringkat
- Antepartum Record Labor WatchDokumen4 halamanAntepartum Record Labor WatchMaryJoy rosalesBelum ada peringkat
- CPG Uti PDFDokumen7 halamanCPG Uti PDFhellokathyyyyyy100% (1)
- General Data: Hannei Lei C. Ung Batch CerebraDokumen9 halamanGeneral Data: Hannei Lei C. Ung Batch CerebraEloiza Jean CustodioBelum ada peringkat
- OPD Adolescent History FormDokumen5 halamanOPD Adolescent History FormNehemiah FranciscoBelum ada peringkat
- Home Against Medical AdviceDokumen1 halamanHome Against Medical AdvicePia VSBelum ada peringkat
- Case RPORT HsyDokumen12 halamanCase RPORT HsyEshaal Khan100% (1)
- IM AdconDokumen28 halamanIM AdconCla SantosBelum ada peringkat
- Department of Pediatrics: Case ProtocolDokumen11 halamanDepartment of Pediatrics: Case ProtocolKim Adarem Joy ManimtimBelum ada peringkat
- Gestational Trophoblastic Disease Pt2Dokumen75 halamanGestational Trophoblastic Disease Pt2Abdullah KesalBelum ada peringkat
- PFC MatrixDokumen48 halamanPFC Matrixjemma chayocasBelum ada peringkat
- 3 Death Registration Legal Mandates Rules and Procedures 0621Dokumen65 halaman3 Death Registration Legal Mandates Rules and Procedures 0621Harrison sajor100% (1)
- Client Information Sheet NCM107Dokumen4 halamanClient Information Sheet NCM107Rolland Ray MendozaBelum ada peringkat
- F.08 Death CertificateDokumen7 halamanF.08 Death CertificateDasha VeeBelum ada peringkat
- Midsayap Doctors Specialist Hospital, Inc.: Clinical Cover SheetDokumen2 halamanMidsayap Doctors Specialist Hospital, Inc.: Clinical Cover SheetRemej SilutgamBelum ada peringkat
- MAM Manual of OperationsDokumen144 halamanMAM Manual of OperationsJames Abram GuardiarioBelum ada peringkat
- OB-0102D-Obstetric History and PEDokumen6 halamanOB-0102D-Obstetric History and PESiselle FajardoBelum ada peringkat
- Comprehensive Adult Health HistoryDokumen7 halamanComprehensive Adult Health HistoryKhirsna PasajolBelum ada peringkat
- Form 5 - Rapid Health Assessment (MCI)Dokumen1 halamanForm 5 - Rapid Health Assessment (MCI)DELIVERY ROOMBelum ada peringkat
- OB History Endorsement FormatDokumen6 halamanOB History Endorsement FormatVin CustodioBelum ada peringkat
- Medicine OB History and PE TemplateDokumen9 halamanMedicine OB History and PE TemplateJanella SuerteBelum ada peringkat
- Pre-Hospital Assessment Sheet: Triage ScoreDokumen2 halamanPre-Hospital Assessment Sheet: Triage Scoreratna purwitasariBelum ada peringkat
- Case Sheet L3Dokumen22 halamanCase Sheet L3Gulfeshan ArshiBelum ada peringkat
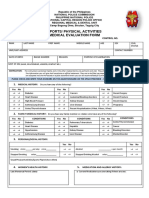
- Pre Medical Evaluatiom Form PFT 1 PDFDokumen2 halamanPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (2)
- Ob-Gyne: Obstetric History and PEDokumen6 halamanOb-Gyne: Obstetric History and PEPorori BookshopBelum ada peringkat
- CPM Benign Prostatic HyperplasiaDokumen7 halamanCPM Benign Prostatic HyperplasiaVon BellosilloBelum ada peringkat
- Doctor's Order Phase 2Dokumen5 halamanDoctor's Order Phase 2Renea Joy ArruejoBelum ada peringkat
- History Taking Form in Gynecology Obstetrics - CompressDokumen8 halamanHistory Taking Form in Gynecology Obstetrics - CompresskeightBelum ada peringkat
- Referral Form Jessa 2021Dokumen1 halamanReferral Form Jessa 2021Jessa MaeBelum ada peringkat
- Mother's Class NutritionDokumen26 halamanMother's Class NutritionRA TranceBelum ada peringkat
- Cagayan de Oro City College of Nursing Assessment FormDokumen12 halamanCagayan de Oro City College of Nursing Assessment Formsticdo_nursing2011Belum ada peringkat
- Family Life CycleDokumen34 halamanFamily Life CycleKathrina AbastarBelum ada peringkat
- Universidad de Manila College of Nursing Community Health Survey ToolDokumen9 halamanUniversidad de Manila College of Nursing Community Health Survey Toolaina_boydonBelum ada peringkat
- Cga - 1Dokumen19 halamanCga - 1Kenji Tolero100% (1)
- Annex B Konsulta ChecklistDokumen8 halamanAnnex B Konsulta ChecklistFret Ramirez Coronia RNBelum ada peringkat
- Philippine General HospitalDokumen5 halamanPhilippine General HospitalMamski AnnBelum ada peringkat
- Post OpDokumen6 halamanPost OpFrinkaWijayaBelum ada peringkat
- Antenatal RecordDokumen2 halamanAntenatal Recordcode4saleBelum ada peringkat
- Hypertension and Diabetes ClubDokumen15 halamanHypertension and Diabetes Clubncd.bulacanBelum ada peringkat
- Diarrhea Concept MapDokumen1 halamanDiarrhea Concept MapIris MambuayBelum ada peringkat
- Mariano Marcos State University: College of Health SciencesDokumen3 halamanMariano Marcos State University: College of Health SciencesJoshua GonzalesBelum ada peringkat
- DILG-DOH-NCIP Joint Circulars On Delivery of Health Services To IPsDokumen18 halamanDILG-DOH-NCIP Joint Circulars On Delivery of Health Services To IPsVincent BautistaBelum ada peringkat
- DOH DM 2019 0062 HepB Demo Project With Interim GuidelinesDokumen31 halamanDOH DM 2019 0062 HepB Demo Project With Interim GuidelinesRold Brio SosBelum ada peringkat
- DengueDokumen5 halamanDengueSam Angelo EstrellaBelum ada peringkat
- National Immunization Program: Manual of Procedures Booklet 8Dokumen28 halamanNational Immunization Program: Manual of Procedures Booklet 8Blue PielagoBelum ada peringkat
- Teenage PregnancyDokumen10 halamanTeenage PregnancyJulymar B.MillareBelum ada peringkat
- Post - Natal Case ProformaDokumen4 halamanPost - Natal Case Proformakavya sriBelum ada peringkat
- Philhealth: Coverage and ExclusionsDokumen15 halamanPhilhealth: Coverage and ExclusionsJoher MendezBelum ada peringkat
- Hippocratic OathDokumen3 halamanHippocratic OathFranckkMnsterBelum ada peringkat
- Pre Authorization FormDokumen1 halamanPre Authorization FormMurugan RamalingamBelum ada peringkat
- Pedia Case ProtocolDokumen5 halamanPedia Case ProtocolAllene PaderangaBelum ada peringkat
- Family Planning: Soledad Chu-Crisostomo, MD, FPOGSDokumen3 halamanFamily Planning: Soledad Chu-Crisostomo, MD, FPOGSColeen NeyraBelum ada peringkat
- GYNE 9 1 Breast Diseases PDFDokumen19 halamanGYNE 9 1 Breast Diseases PDFColeen NeyraBelum ada peringkat
- Psoriasis: Case Management ConferenceDokumen62 halamanPsoriasis: Case Management ConferenceColeen NeyraBelum ada peringkat
- Antibiotic Therapy For Diabetic Foot Infection Tonnerre PDFDokumen61 halamanAntibiotic Therapy For Diabetic Foot Infection Tonnerre PDFColeen NeyraBelum ada peringkat
- Patient's Name: Pedia: Mother's Name: OB-Gyne: Room: Blood Type: Date of Birth: JI In-Charge: Time of Birth: Admitting Notes I. General DataDokumen2 halamanPatient's Name: Pedia: Mother's Name: OB-Gyne: Room: Blood Type: Date of Birth: JI In-Charge: Time of Birth: Admitting Notes I. General DataColeen NeyraBelum ada peringkat
- Principles of Development:: Supplemental Handout # 2: Developmental AssessmentDokumen6 halamanPrinciples of Development:: Supplemental Handout # 2: Developmental AssessmentColeen NeyraBelum ada peringkat
- Bioethics PDFDokumen117 halamanBioethics PDFColeen NeyraBelum ada peringkat
- WARDWORK TemplateDokumen9 halamanWARDWORK TemplateColeen NeyraBelum ada peringkat
- Stainless Steel Crowns PDFDokumen4 halamanStainless Steel Crowns PDFLuciaTrinovenaLaseBelum ada peringkat
- Group 2:: Assignment: 01 Subject: Operations ManagementDokumen5 halamanGroup 2:: Assignment: 01 Subject: Operations Managementmy VinayBelum ada peringkat
- By: Socorro Milagros C. Alcancia, RND, MBADokumen35 halamanBy: Socorro Milagros C. Alcancia, RND, MBAJerico RiveraBelum ada peringkat
- Kegawatdaruratan Otak (Siloam - 14 Mei 2008)Dokumen34 halamanKegawatdaruratan Otak (Siloam - 14 Mei 2008)Ruki HartawanBelum ada peringkat
- Committee Report Brgy Ordinance - For ScribdDokumen2 halamanCommittee Report Brgy Ordinance - For ScribdJoshelle B. Bancilo100% (3)
- Atlas WebDokumen126 halamanAtlas WebsnehBelum ada peringkat
- U9W6 - Physiology of LactationDokumen2 halamanU9W6 - Physiology of LactationSuh KhaBelum ada peringkat
- Medicine Brochure Entry 2019 PDFDokumen30 halamanMedicine Brochure Entry 2019 PDFRevathi VaisnaveeBelum ada peringkat
- Signal Review Panel Under PvPI PDFDokumen3 halamanSignal Review Panel Under PvPI PDFAnju ThejkumarBelum ada peringkat
- DR Mercola - How Are The COVID Shots Affecting Mothers-To-BeDokumen10 halamanDR Mercola - How Are The COVID Shots Affecting Mothers-To-Beguy777Belum ada peringkat
- Betz Rebecca ResumeDokumen2 halamanBetz Rebecca Resumeapi-316054946Belum ada peringkat
- Fast Hugs MaidenDokumen8 halamanFast Hugs MaidenPriscila Navarro MedinaBelum ada peringkat
- DynaMed Plus - Pulmonary Embolism (PE)Dokumen85 halamanDynaMed Plus - Pulmonary Embolism (PE)Gamer MadaBelum ada peringkat
- Challenging Concepts in INTERVENTIONAL RADIOLOGY 1st EditionDokumen363 halamanChallenging Concepts in INTERVENTIONAL RADIOLOGY 1st EditionHisham Elkilaney100% (1)
- The Abington Journal 10-03-2012Dokumen22 halamanThe Abington Journal 10-03-2012The Times LeaderBelum ada peringkat
- P2010/0509-001 Management of EclampsiaDokumen7 halamanP2010/0509-001 Management of EclampsiaYwagar YwagarBelum ada peringkat
- Congenital Heart DiseaseDokumen2 halamanCongenital Heart Diseasejhayviec0% (1)
- Morning Report PSPDokumen9 halamanMorning Report PSPJessicaBelum ada peringkat
- Peter 2Dokumen1.324 halamanPeter 2Vansh Dutt100% (1)
- Ethical Issues in Nursing PracticeDokumen10 halamanEthical Issues in Nursing PracticeP'Babe Cece Adumoah0% (1)
- Ob Gynsmhobjectivesfinal PDFDokumen4 halamanOb Gynsmhobjectivesfinal PDFhanzukikBelum ada peringkat
- 6 Pregnancy Related Terms 30-04-2020Dokumen12 halaman6 Pregnancy Related Terms 30-04-2020DaniJaralBelum ada peringkat
- Selective Pressure Impressions Methods PDFDokumen3 halamanSelective Pressure Impressions Methods PDFAgus PudiantoBelum ada peringkat
- Rockaway Times 11818Dokumen40 halamanRockaway Times 11818Peter J. MahonBelum ada peringkat
- Kids Box For Spanish Speakers 4Dokumen10 halamanKids Box For Spanish Speakers 4Laura BaBoBelum ada peringkat
- Sdn-Cuban PolyclinicDokumen23 halamanSdn-Cuban PolyclinicMaria Socorro AlcantaraBelum ada peringkat
- Classification of Pediatric Urinary Tract DilationDokumen7 halamanClassification of Pediatric Urinary Tract DilationYaroshlav Gonzalez DoradoBelum ada peringkat
- Usability Testing of Instructions For Use For Cleaning, Disinfection and Sterilization of Ultrasound ProbesDokumen9 halamanUsability Testing of Instructions For Use For Cleaning, Disinfection and Sterilization of Ultrasound Probespolish001Belum ada peringkat
- Tosp Booklet With MSP (3 Jan 2017) WordDokumen112 halamanTosp Booklet With MSP (3 Jan 2017) WordArif Tri Prasetyo HarunBelum ada peringkat