Anda mungkin juga menyukai
- ScriptDokumen12 halamanScriptWaleed Nadeem50% (2)
- Pathophysiology SARSDokumen4 halamanPathophysiology SARSStephanie Joy Escala71% (7)
- Counselling LetterDokumen1 halamanCounselling LetterSeann LorescoBelum ada peringkat
- MannitolDokumen3 halamanMannitolAlexandra AntondyBelum ada peringkat
- Drug StudyDokumen5 halamanDrug StudyGAYOL BREEN IRAH A.Belum ada peringkat
- Precipitating Factor Predisposing FactorsDokumen1 halamanPrecipitating Factor Predisposing FactorsanthropusBelum ada peringkat
- Dental Prob NCPDokumen3 halamanDental Prob NCPx483xDBelum ada peringkat
- NCP OsteosarcomaDokumen6 halamanNCP OsteosarcomaNiksBelum ada peringkat
- Schematic Diagram BA HAP HRDokumen2 halamanSchematic Diagram BA HAP HRMika MinsalanBelum ada peringkat
- 100QforCIP 30QforDiagnosticReviewDokumen29 halaman100QforCIP 30QforDiagnosticReviewpamgelBelum ada peringkat
- Psych - Chapter 23 Into To Milieu ManagementDokumen4 halamanPsych - Chapter 23 Into To Milieu ManagementKaren かれんBelum ada peringkat
- Nursing AssessmentDokumen4 halamanNursing AssessmentFlor SabaysabayBelum ada peringkat
- Burn - Daily Physical AssessmentDokumen8 halamanBurn - Daily Physical AssessmentkrishcelBelum ada peringkat
- SLE PathophysiologyDokumen3 halamanSLE PathophysiologyyasiraBelum ada peringkat
- Drug Study Domperidone CompressDokumen1 halamanDrug Study Domperidone CompressAngelica TolledoBelum ada peringkat
- Nursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionDokumen2 halamanNursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionTammy De GuzmanBelum ada peringkat
- FINALS ReviewerDokumen14 halamanFINALS ReviewerJustine Simeon lagunzadBelum ada peringkat
- PathophysiologyDokumen9 halamanPathophysiologySuzette PipoBelum ada peringkat
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDokumen2 halamanName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesIvan Matthew SuperioBelum ada peringkat
- Acute Pain NCPDokumen2 halamanAcute Pain NCPfbarlicosBelum ada peringkat
- Running Head: Comprehensive Case Study 1Dokumen11 halamanRunning Head: Comprehensive Case Study 1api-546355462Belum ada peringkat
- Prioritization of Problems Health Problem:: Carlatan, San Fernando City, La UnionDokumen4 halamanPrioritization of Problems Health Problem:: Carlatan, San Fernando City, La UnionGabrielle John HernaezBelum ada peringkat
- ASSESSMENTDokumen2 halamanASSESSMENTColeen PequitBelum ada peringkat
- 51 100Dokumen18 halaman51 100Jaessa Feliciano100% (1)
- Cefadroxil DuricefDokumen1 halamanCefadroxil Duricefstaylor235Belum ada peringkat
- HERNIADokumen27 halamanHERNIAVanessa SumalbagBelum ada peringkat
- Huntingtons Disease NCPDokumen4 halamanHuntingtons Disease NCPJerich Mark SalasBelum ada peringkat
- Pathophysiology of Severe AnemiaDokumen3 halamanPathophysiology of Severe AnemiaChrizley Shawn DeroniaBelum ada peringkat
- BARANDINO, Jia Laurice (Gouty Arthritis)Dokumen18 halamanBARANDINO, Jia Laurice (Gouty Arthritis)Deinielle Magdangal RomeroBelum ada peringkat
- Psych NCPDokumen4 halamanPsych NCPnoman-053Belum ada peringkat
- AppendectomyDokumen35 halamanAppendectomyleighjagBelum ada peringkat
- Surgical InstrumentDokumen5 halamanSurgical Instrumentria_soriano_2100% (1)
- Pneumonia PathoDokumen2 halamanPneumonia PathoDerick Nyl PascualBelum ada peringkat
- Electrical Burn PathophysiologyDokumen1 halamanElectrical Burn PathophysiologydanicaBelum ada peringkat
- LFDDokumen3 halamanLFDVhince Norben PiscoBelum ada peringkat
- Attapulgite PDFDokumen1 halamanAttapulgite PDFWindy Tonapa100% (1)
- Pathophysiology, Bone CancerDokumen7 halamanPathophysiology, Bone CancerMaria Grace Raquel Ormeneta100% (1)
- Movie Wit Scholarly AssignmentDokumen10 halamanMovie Wit Scholarly Assignmentapi-283868512Belum ada peringkat
- CiprobayDokumen2 halamanCiprobayianecunar100% (1)
- Activity 6 - Drug StudyDokumen14 halamanActivity 6 - Drug StudyAl-Mujib TanogBelum ada peringkat
- Pathophysiology of Pediculosis CapitisDokumen1 halamanPathophysiology of Pediculosis CapitisAldrin Ian Oraza Alpe0% (1)
- Pathophysiology Cholelithiasis 2Dokumen2 halamanPathophysiology Cholelithiasis 2Jamie HaravataBelum ada peringkat
- Drug Study EditedDokumen5 halamanDrug Study EditedfabtaciousVeelaBelum ada peringkat
- PYOMYOSITISDokumen6 halamanPYOMYOSITISChristine CoridoBelum ada peringkat
- Essay 1Dokumen2 halamanEssay 1Geraldine ArellanoBelum ada peringkat
- Pathophysiology of Multiple Myeloma OkDokumen3 halamanPathophysiology of Multiple Myeloma OkRifa'atul MahmudahBelum ada peringkat
- FNCP Final FinalDokumen51 halamanFNCP Final FinalMichael Piduca100% (1)
- Self-Care Deficit Related To Inability To Perceive Body Part (Bathing)Dokumen2 halamanSelf-Care Deficit Related To Inability To Perceive Body Part (Bathing)lilpeabea100% (1)
- MyelomeningoceleDokumen7 halamanMyelomeningocelemavefigBelum ada peringkat
- Annotated Group 2 Impetigo Concept Mapping 1Dokumen30 halamanAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANOBelum ada peringkat
- Content: Outline Form Only Make A Separate Sheet For The Content. The Health Teaching Plan Should Focus On Home Care For Patients With Mood DisorderDokumen4 halamanContent: Outline Form Only Make A Separate Sheet For The Content. The Health Teaching Plan Should Focus On Home Care For Patients With Mood DisorderRaffy Sebastian Seballos100% (1)
- (Brand Name) & Date Ordered General Class and Family Specific IndicationDokumen2 halaman(Brand Name) & Date Ordered General Class and Family Specific IndicationNicole Grace VillegasBelum ada peringkat
- Nursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursDokumen4 halamanNursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursRawan KhateebBelum ada peringkat
- Acute Gastroenteritis With Severe DehydrationDokumen22 halamanAcute Gastroenteritis With Severe DehydrationCess Dunwan100% (1)
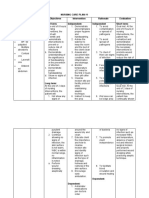
- Nursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermDokumen5 halamanNursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermAlmer OstreaBelum ada peringkat
- CASE STUDY (Gastro)Dokumen3 halamanCASE STUDY (Gastro)Jake Yvan DizonBelum ada peringkat
- Management of Tuberculosis: A guide for clinicians (eBook edition)Dari EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Belum ada peringkat
- Illustrator File Edit Select Effect View Window HelpDokumen8 halamanIllustrator File Edit Select Effect View Window HelpHaizel BieberBelum ada peringkat
- Ear DisorderDokumen61 halamanEar DisorderSakthi DeviBelum ada peringkat
- Luz Farms V Sec of DarDokumen9 halamanLuz Farms V Sec of DarJoe RealBelum ada peringkat
- People v. MadragaDokumen2 halamanPeople v. MadragaJoe RealBelum ada peringkat
- Sharp Int Market V CA +LBP & VistanDokumen7 halamanSharp Int Market V CA +LBP & VistanJoe RealBelum ada peringkat
- Rivera-Calingasan V RiveraDokumen8 halamanRivera-Calingasan V RiveraJoe RealBelum ada peringkat
- Title Vi - Usufruct Chapter One: Usufruct in General: Property NotesDokumen16 halamanTitle Vi - Usufruct Chapter One: Usufruct in General: Property NotesJoe RealBelum ada peringkat
- Gaboya V CuiDokumen11 halamanGaboya V CuiJoe RealBelum ada peringkat
- Moralidad V Sps PernesDokumen8 halamanMoralidad V Sps PernesJoe RealBelum ada peringkat
- Asis v. Minister of LaborDokumen4 halamanAsis v. Minister of LaborJoe RealBelum ada peringkat
- Royal Plant Workers Union v. Coca Cola BottlersDokumen5 halamanRoyal Plant Workers Union v. Coca Cola BottlersJoe RealBelum ada peringkat
- Taglay v. Judge Trabajo Daray DigestDokumen2 halamanTaglay v. Judge Trabajo Daray DigestJoe RealBelum ada peringkat
- 3 (6) Baluran V NavarroDokumen6 halaman3 (6) Baluran V NavarroJoe RealBelum ada peringkat
- American Wire and Cable Daily Rated Employees Union v. American Wire and CableDokumen11 halamanAmerican Wire and Cable Daily Rated Employees Union v. American Wire and CableJoe RealBelum ada peringkat
- Teng v. PahagacDokumen13 halamanTeng v. PahagacJoe RealBelum ada peringkat
- St. Mary's University v. CA, March 8, 2005Dokumen6 halamanSt. Mary's University v. CA, March 8, 2005Joe RealBelum ada peringkat
- 15 Nestle Philippines, Inc. v. Puedan, JR.Dokumen4 halaman15 Nestle Philippines, Inc. v. Puedan, JR.Joe RealBelum ada peringkat
- 13 (10) Manila Memorial Park Cemetery v. LuizDokumen3 halaman13 (10) Manila Memorial Park Cemetery v. LuizJoe RealBelum ada peringkat
- Exodus International Construction v. Biscocho, February 23, 2011Dokumen11 halamanExodus International Construction v. Biscocho, February 23, 2011Joe RealBelum ada peringkat
- First Division G.R. No. 193493, June 13, 2013: Supreme Court of The PhilippinesDokumen15 halamanFirst Division G.R. No. 193493, June 13, 2013: Supreme Court of The PhilippinesJoe RealBelum ada peringkat
- Poseidon Fishing v. NLRC, February 20, 2006Dokumen14 halamanPoseidon Fishing v. NLRC, February 20, 2006Joe RealBelum ada peringkat
- de La Salle University Araneta v. Bernardo, February 13, 2017Dokumen17 halamande La Salle University Araneta v. Bernardo, February 13, 2017Joe RealBelum ada peringkat
- Pldt-vs-Arceo-digestDokumen3 halamanPldt-vs-Arceo-digestJoe RealBelum ada peringkat
- Mingoa V LRADokumen4 halamanMingoa V LRAJoe RealBelum ada peringkat
- Case Digest LaborDokumen2 halamanCase Digest LaborJoe RealBelum ada peringkat
- Florencio Ignao Vs IacDokumen1 halamanFlorencio Ignao Vs IacJoe RealBelum ada peringkat
- 12 (19) Diamond Farms v. Farms Agrarian Reform Beneficiaries Multi-Purpose CooperativeDokumen19 halaman12 (19) Diamond Farms v. Farms Agrarian Reform Beneficiaries Multi-Purpose CooperativeJoe RealBelum ada peringkat
- San Miguel Corporation Vs AballaDokumen4 halamanSan Miguel Corporation Vs AballaJoe RealBelum ada peringkat
- Meralco Industrial Engineering Services v. NLRCDokumen5 halamanMeralco Industrial Engineering Services v. NLRCJoe RealBelum ada peringkat
- Pardell V BartolomeDokumen1 halamanPardell V BartolomeJoe RealBelum ada peringkat
- Sales Case ListDokumen6 halamanSales Case ListJoe RealBelum ada peringkat
- PAL v. Ligan (G.R. No. 146408) : Investment Which Relates To The Job, Work or Service To BeDokumen3 halamanPAL v. Ligan (G.R. No. 146408) : Investment Which Relates To The Job, Work or Service To BeJoe RealBelum ada peringkat
- 429-Article Text-1894-2-10-20210715Dokumen12 halaman429-Article Text-1894-2-10-20210715Ziya AstgaBelum ada peringkat
- African National Congress: Department of Information and PublicityDokumen9 halamanAfrican National Congress: Department of Information and PublicityeNCA.com100% (2)
- Body Template 1998Dokumen7 halamanBody Template 1998itayBelum ada peringkat
- 10 1007@s00068-mfjrbtDokumen14 halaman10 1007@s00068-mfjrbtJGunar VasquezBelum ada peringkat
- Professional Review Industry Route Guidance NotesDokumen10 halamanProfessional Review Industry Route Guidance NotesAnonymous TlYmhkBelum ada peringkat
- Meditation ScriptDokumen9 halamanMeditation Scriptapi-361293242100% (1)
- Child Welfare Trauma Training Participant GuideDokumen104 halamanChild Welfare Trauma Training Participant GuideAllison PalmisanoBelum ada peringkat
- Shape Up BusyBee CarysDokumen16 halamanShape Up BusyBee CarysElena HorodincaBelum ada peringkat
- Survey QuestionnaireDokumen2 halamanSurvey Questionnairecyrusbatayan100% (1)
- MSDS PDFDokumen5 halamanMSDS PDFdang2172014Belum ada peringkat
- Colorado Department of Public Health and Environment: November 14 Public-Health Order UpdateDokumen9 halamanColorado Department of Public Health and Environment: November 14 Public-Health Order UpdateMichael_Roberts2019Belum ada peringkat
- Fractures NoteDokumen31 halamanFractures NoteNoor AlblushiBelum ada peringkat
- Allocating Hospital Resources To Improve Patient ExperienceDokumen6 halamanAllocating Hospital Resources To Improve Patient ExperienceMichael0% (1)
- 2022 Projects City of BethlehemDokumen17 halaman2022 Projects City of BethlehemLVNewsdotcomBelum ada peringkat
- 3 5 18 950 PDFDokumen3 halaman3 5 18 950 PDFBang AthanBelum ada peringkat
- Clinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDokumen9 halamanClinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpSiva SubramaniamBelum ada peringkat
- Hematinics: Dr. Monalisa Mondal Demonstrator Department of PharmacologyDokumen28 halamanHematinics: Dr. Monalisa Mondal Demonstrator Department of PharmacologyShirsh JauriharBelum ada peringkat
- Labor and Delivery OB Concept MapDokumen2 halamanLabor and Delivery OB Concept MapMissy Johnson75% (4)
- Designated Structural Engineer Final 2016Dokumen4 halamanDesignated Structural Engineer Final 2016Sri KalyanBelum ada peringkat
- Nahom ShewangizawDokumen38 halamanNahom Shewangizawawel centerBelum ada peringkat
- Jdo Vol 59 New PDFDokumen100 halamanJdo Vol 59 New PDFLex MBelum ada peringkat
- 5AB 783651 CompleteBook R39 Jan12Dokumen146 halaman5AB 783651 CompleteBook R39 Jan12Gdb HasseneBelum ada peringkat
- Lecture #3 - Carbohydrates & LipidsDokumen23 halamanLecture #3 - Carbohydrates & Lipidsogangurel100% (3)
- CircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesDokumen43 halamanCircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesMenaBelum ada peringkat
- Interval TrainingDokumen24 halamanInterval TrainingRukmantaraBelum ada peringkat
- Mms Health Recovery Guidebook 1 October 2016Dokumen346 halamanMms Health Recovery Guidebook 1 October 2016omar hazard94% (50)
- Book of Best Practices Trauma and The Role of Mental Health in Post-Conflict RecoveryDokumen383 halamanBook of Best Practices Trauma and The Role of Mental Health in Post-Conflict RecoveryDiego Salcedo AvilaBelum ada peringkat
- 01 EnemaDokumen4 halaman01 Enemabunso padillaBelum ada peringkat
- Abdominal PainDokumen39 halamanAbdominal PainIsma Resti PratiwiBelum ada peringkat
- SPS and TBT MeasuresDokumen4 halamanSPS and TBT MeasuresValentina Vasquez CasallasBelum ada peringkat