Anda mungkin juga menyukai
- Peripheral Vascular Disease Surgical PresentationDokumen26 halamanPeripheral Vascular Disease Surgical PresentationqreenBelum ada peringkat
- VSIM Nursing Clinical Rotation WorksheetDokumen13 halamanVSIM Nursing Clinical Rotation WorksheetVin Lorenzo CampbellBelum ada peringkat
- Antepartum Record Labor WatchDokumen4 halamanAntepartum Record Labor WatchMaryJoy rosalesBelum ada peringkat
- Salbutamol Drug SummDokumen1 halamanSalbutamol Drug SummWarren100% (2)
- Epinephrine and Dexamethasone in Children With BronchiolitisDokumen11 halamanEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisBelum ada peringkat
- OSCE Final 1 PDFDokumen204 halamanOSCE Final 1 PDFamalBelum ada peringkat
- Brain Cancer ReportDokumen5 halamanBrain Cancer ReportCrisantaCasliBelum ada peringkat
- Understanding Hemangiomas: Causes, Types and TreatmentsDokumen18 halamanUnderstanding Hemangiomas: Causes, Types and Treatmentsplastic guardiansBelum ada peringkat
- Boli Digestive Functionale 2018Dokumen90 halamanBoli Digestive Functionale 2018Cabel TeodorBelum ada peringkat
- Tachypnoea Predicts Hypoxia in Acutely Ill InfantsDokumen5 halamanTachypnoea Predicts Hypoxia in Acutely Ill Infantsselli novita belindaBelum ada peringkat
- Hypoxemia in Children With Pneumonia and Its Clinical PredictorsDokumen6 halamanHypoxemia in Children With Pneumonia and Its Clinical Predictorsamalia chairunnisaBelum ada peringkat
- Tachypnea Is A Useful Predictor of Pneumonia in Children With Acute Respiratory InfectionDokumen2 halamanTachypnea Is A Useful Predictor of Pneumonia in Children With Acute Respiratory InfectionAli BabaBelum ada peringkat
- Newborn Respiratory Distress CausesDokumen5 halamanNewborn Respiratory Distress CausesNovia KurniantiBelum ada peringkat
- 2174 8646 1 PBDokumen5 halaman2174 8646 1 PBKiran PantheeBelum ada peringkat
- Buonsenso Et Al-2018-Pediatric PulmonologyDokumen9 halamanBuonsenso Et Al-2018-Pediatric Pulmonologywawa chenBelum ada peringkat
- Lung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFDokumen8 halamanLung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFcesar juarezBelum ada peringkat
- Jurnal Pubme 1 RdsDokumen13 halamanJurnal Pubme 1 Rdsriri risna aBelum ada peringkat
- Diagnosis of Pneumonia in Children With Dehydrating DiarrhoeaDokumen6 halamanDiagnosis of Pneumonia in Children With Dehydrating DiarrhoeaEmaa AmooraBelum ada peringkat
- A Radiological Perspective of Assessing Neonatal Respiratory Distress SyndromeDokumen6 halamanA Radiological Perspective of Assessing Neonatal Respiratory Distress Syndromeyoga zunandy pratamaBelum ada peringkat
- Contoh Tesis NMJ 56 287Dokumen5 halamanContoh Tesis NMJ 56 287Lidwina ElisabethBelum ada peringkat
- Ppul 24811Dokumen5 halamanPpul 24811rizki romadaniBelum ada peringkat
- IJP Volume 6 Issue 11 Pages 8507-8516Dokumen10 halamanIJP Volume 6 Issue 11 Pages 8507-8516Marda LinaBelum ada peringkat
- Artigo Ana e Frederico 2021Dokumen10 halamanArtigo Ana e Frederico 2021CarolinaBelum ada peringkat
- Ajrcccm 2004Dokumen9 halamanAjrcccm 2004kichilla1Belum ada peringkat
- BMJ c4978 FullDokumen6 halamanBMJ c4978 Fulljesusm_115Belum ada peringkat
- Periodic Breathing and Apnea in Preterm InfantsDokumen4 halamanPeriodic Breathing and Apnea in Preterm InfantsIvan VeriswanBelum ada peringkat
- Viral Respiratory Infections in Preterm Infants During andDokumen9 halamanViral Respiratory Infections in Preterm Infants During andMariusBelum ada peringkat
- 566-Article Text-2161-3-10-20210707Dokumen6 halaman566-Article Text-2161-3-10-20210707Prashant KoiralaBelum ada peringkat
- Efecto Del Surfatante Menos Invasivo Sobre La Oxigenación CerebralDokumen9 halamanEfecto Del Surfatante Menos Invasivo Sobre La Oxigenación CerebralRonald MoralesBelum ada peringkat
- Infant Breathing and Hypoxia DiagnosisDokumen14 halamanInfant Breathing and Hypoxia DiagnosisAdi Ck Razqa PSBelum ada peringkat
- Articulo Tesis 9Dokumen8 halamanArticulo Tesis 9Lourdes MarcosBelum ada peringkat
- Human Metapneumovirus Associated Pneumonia and Severe Bronchiolitis in A 9-Month-Old Infant Admitted To A Sri Lankan HospitalDokumen5 halamanHuman Metapneumovirus Associated Pneumonia and Severe Bronchiolitis in A 9-Month-Old Infant Admitted To A Sri Lankan HospitalVijayakanth VijayakumarBelum ada peringkat
- SA PerformanceDokumen8 halamanSA Performancefernin96Belum ada peringkat
- VAP Incidence, Risk Factors and Bacteria in PICUDokumen6 halamanVAP Incidence, Risk Factors and Bacteria in PICURabiatul 'raney' AdawiyahBelum ada peringkat
- Tto Crup NatureDokumen7 halamanTto Crup NatureCarolina Mora RuedaBelum ada peringkat
- Pneumopericardium Pneumomediastinum and Pneumorrachis in VRS BronchiolitisDokumen4 halamanPneumopericardium Pneumomediastinum and Pneumorrachis in VRS BronchiolitisAbi CardenasBelum ada peringkat
- saul salamat RDSDokumen6 halamansaul salamat RDShoneyailbhatti53Belum ada peringkat
- Effectiveness of Airway ClearanceDokumen7 halamanEffectiveness of Airway ClearanceNelly Lutfieta SariBelum ada peringkat
- Hyperbilirubinemia, Phototherapy, and Childhood Asthma: ObjectivesDokumen11 halamanHyperbilirubinemia, Phototherapy, and Childhood Asthma: ObjectivesrizaniaBelum ada peringkat
- Risks and Outcomes of Infants with Transient Tachypnea of the NewbornDokumen5 halamanRisks and Outcomes of Infants with Transient Tachypnea of the NewbornVerushka CrespoBelum ada peringkat
- Nebul Nacl 3Dokumen7 halamanNebul Nacl 3Arif RSBelum ada peringkat
- Vol-2 Issue-1 Approach To Respiratory Distress in The Newborn 19Dokumen13 halamanVol-2 Issue-1 Approach To Respiratory Distress in The Newborn 19salamredBelum ada peringkat
- Tugas Jurnal Junior Stase RespirologiDokumen44 halamanTugas Jurnal Junior Stase RespirologiIrenaBelum ada peringkat
- Bronchiolitis High Risk ApneaDokumen7 halamanBronchiolitis High Risk ApneaclikgoBelum ada peringkat
- Pediatric Pulmonology 2021, Dell'ortoDokumen8 halamanPediatric Pulmonology 2021, Dell'ortoRadu CiprianBelum ada peringkat
- Sol Hipert en SibilanciasDokumen9 halamanSol Hipert en Sibilanciasedith sandovalBelum ada peringkat
- 26-05-2020-1590469891-8-IJANS-10. IJANS - The Effect of Prone Position Versus Supine Position On Oxygen Saturation Among Jordanian PretermDokumen6 halaman26-05-2020-1590469891-8-IJANS-10. IJANS - The Effect of Prone Position Versus Supine Position On Oxygen Saturation Among Jordanian Pretermiaset123Belum ada peringkat
- Study of Different Treatment Modalities and Outcome in Preterm Babies With Respiratory Distress Syndrome 2017Dokumen4 halamanStudy of Different Treatment Modalities and Outcome in Preterm Babies With Respiratory Distress Syndrome 2017Vita DesriantiBelum ada peringkat
- NakatoIJP Volume6 Issue9 Pages8215-8223Dokumen9 halamanNakatoIJP Volume6 Issue9 Pages8215-8223Siti HumairahBelum ada peringkat
- Observer agreement for respiratory signs and oximetry in infants with lower respiratory infectionsDokumen4 halamanObserver agreement for respiratory signs and oximetry in infants with lower respiratory infectionsIvan VeriswanBelum ada peringkat
- Diagnostic Value of Gastric Shake Test For Hyaline Membrane Disease in Preterm InfantDokumen6 halamanDiagnostic Value of Gastric Shake Test For Hyaline Membrane Disease in Preterm InfantNovia KurniantiBelum ada peringkat
- Best Practice of Pneumonia Management in Pandemic Era: Retno Asih SetyoningrumDokumen48 halamanBest Practice of Pneumonia Management in Pandemic Era: Retno Asih SetyoningrumNurul aina MardhiyahBelum ada peringkat
- Pi Is 1875957219305510Dokumen10 halamanPi Is 1875957219305510madimadi11Belum ada peringkat
- High Flow Oxygen Therapy V Standard Care in InfantsDokumen5 halamanHigh Flow Oxygen Therapy V Standard Care in InfantsJaque ArandaBelum ada peringkat
- Journal Homepage: - : IntroductionDokumen5 halamanJournal Homepage: - : IntroductionIJAR JOURNALBelum ada peringkat
- Art Efecto de Tto Atb en Crecimiento en Terneros Con DX de NeumoniaDokumen13 halamanArt Efecto de Tto Atb en Crecimiento en Terneros Con DX de NeumoniaAndres Alejandro CoralBelum ada peringkat
- Efficacy of Bronchoalveolar Lavage As Adjunct Therapy in The Treatment of Neonatal Severe PneumoniaDokumen6 halamanEfficacy of Bronchoalveolar Lavage As Adjunct Therapy in The Treatment of Neonatal Severe Pneumoniaanita awBelum ada peringkat
- Apid 8 2 98735Dokumen5 halamanApid 8 2 98735ko naythweBelum ada peringkat
- Clinical and epidemiological manifestations of parainfluenza infection in hospitalized childrenDokumen7 halamanClinical and epidemiological manifestations of parainfluenza infection in hospitalized childrenPedroCastroAriasBelum ada peringkat
- Impact of Cesarean Section On Transient TachypneaDokumen7 halamanImpact of Cesarean Section On Transient Tachypneab40284283Belum ada peringkat
- 2010 Early CPAP Vs Surfactant in EPTI NEJMDokumen10 halaman2010 Early CPAP Vs Surfactant in EPTI NEJMFiorella VilcaBelum ada peringkat
- WRIGHT 2016_Continuous Positive Airway Pressure to Prevent Neonatal Lung InjuryDokumen10 halamanWRIGHT 2016_Continuous Positive Airway Pressure to Prevent Neonatal Lung InjuryRafael JustinoBelum ada peringkat
- A Review of Normal Values of Infant Sleep PolysomnographyDokumen6 halamanA Review of Normal Values of Infant Sleep PolysomnographyGil CLBelum ada peringkat
- Jnksreenan 2001Dokumen5 halamanJnksreenan 2001fitriBelum ada peringkat
- Childhood Community Acquired Pneumonia A Review of Etiology and Antimicrobial Treatment Studies.Dokumen10 halamanChildhood Community Acquired Pneumonia A Review of Etiology and Antimicrobial Treatment Studies.Andry Wahyudi AgusBelum ada peringkat
- A Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisDokumen11 halamanA Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisErwin YanthoBelum ada peringkat
- News in SurgeryDokumen9 halamanNews in Surgerymuthia khairunnisaBelum ada peringkat
- Case ReportDokumen5 halamanCase Reportmuthia khairunnisaBelum ada peringkat
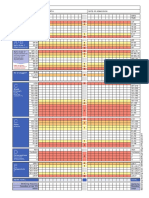
- NEWS2 Chart 3 - NEWS Observation Chart - 0Dokumen1 halamanNEWS2 Chart 3 - NEWS Observation Chart - 0muthia khairunnisaBelum ada peringkat
- Kjim 2016 360Dokumen11 halamanKjim 2016 360berriandi_arwanBelum ada peringkat
- Neonatal Sepsis Highlighting The Principles of Dia PDFDokumen5 halamanNeonatal Sepsis Highlighting The Principles of Dia PDFmuthia khairunnisaBelum ada peringkat
- News in SurgeryDokumen9 halamanNews in Surgerymuthia khairunnisaBelum ada peringkat
- Physical Examination Vascular System: of TheDokumen63 halamanPhysical Examination Vascular System: of TheyuniayuuuBelum ada peringkat
- Tutor A21Dokumen8 halamanTutor A21muthia khairunnisaBelum ada peringkat
- Chart 1: The NEWS scoring system for vital signsDokumen1 halamanChart 1: The NEWS scoring system for vital signsFlouria Stefanny SimatupangBelum ada peringkat
- Review Article: Postcoital Bleeding: A Review On Etiology, Diagnosis, and ManagementDokumen9 halamanReview Article: Postcoital Bleeding: A Review On Etiology, Diagnosis, and ManagementAnonymous i9mBoeOuBelum ada peringkat
- Jurnal EKG Abnormal Arif Rahman HakimDokumen8 halamanJurnal EKG Abnormal Arif Rahman Hakimmuthia khairunnisaBelum ada peringkat
- Teknik Sungai Dan Rawa-05Dokumen60 halamanTeknik Sungai Dan Rawa-05muthia khairunnisaBelum ada peringkat
- SPSSDokumen5 halamanSPSSmuthia khairunnisaBelum ada peringkat
- Viral MeningitisDokumen6 halamanViral Meningitismuthia khairunnisaBelum ada peringkat
- Lampiran Perhitungan Bab IvDokumen5 halamanLampiran Perhitungan Bab Ivmuthia khairunnisaBelum ada peringkat
- Laporan Tugas Pengenalan Profesi Blok Xvi Sistem Sensoris Dan Integumentum "Identifikasi Gangguan Pendengaran Di Ypac"Dokumen1 halamanLaporan Tugas Pengenalan Profesi Blok Xvi Sistem Sensoris Dan Integumentum "Identifikasi Gangguan Pendengaran Di Ypac"muthia khairunnisaBelum ada peringkat
- Art 40930 PDFDokumen13 halamanArt 40930 PDFBrahma MishraBelum ada peringkat
- MUBESDokumen2 halamanMUBESmuthia khairunnisaBelum ada peringkat
- 1.c. What's The Impact of Shortness of Breath? AnswerDokumen7 halaman1.c. What's The Impact of Shortness of Breath? Answermuthia khairunnisaBelum ada peringkat
- Jawaban Hakim Sken ADokumen3 halamanJawaban Hakim Sken Amuthia khairunnisaBelum ada peringkat
- Laporan Penanggungjawaban Lomba Cepat Tepat Spices 2018 FK Um PalembangDokumen1 halamanLaporan Penanggungjawaban Lomba Cepat Tepat Spices 2018 FK Um Palembangmuthia khairunnisaBelum ada peringkat
- Choosing Between Colloids and Crystalloids For IV InfusionDokumen4 halamanChoosing Between Colloids and Crystalloids For IV InfusionFamily Prepper100% (1)
- Total XVDokumen8 halamanTotal XVMohammed HaiderBelum ada peringkat
- Magna Carta: Republic Act 7305: Magna Carta of Public Health WorkersDokumen50 halamanMagna Carta: Republic Act 7305: Magna Carta of Public Health WorkersZyrene RiveraBelum ada peringkat
- Assignment - EugenicsDokumen11 halamanAssignment - EugenicsNavneet GillBelum ada peringkat
- Anti TB PPT FinalDokumen43 halamanAnti TB PPT FinalKeziah GillBelum ada peringkat
- Risk Factors in Dental ErosionDokumen6 halamanRisk Factors in Dental ErosionMuftihat IsrarBelum ada peringkat
- EDokumen375 halamanEANA MARIA CRISTIANABelum ada peringkat
- FNCP List of 1st Level AssessmentDokumen6 halamanFNCP List of 1st Level AssessmentReignallienn Inocencio MartinBelum ada peringkat
- Training English Individual Task Lecturers: Umi Rachmawati, M.PDDokumen14 halamanTraining English Individual Task Lecturers: Umi Rachmawati, M.PDVeni UNBelum ada peringkat
- How To Fill ADR Reporitng Form and Causality AssessmentDokumen38 halamanHow To Fill ADR Reporitng Form and Causality AssessmentVishal AryaBelum ada peringkat
- "Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADokumen21 halaman"Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADimple AnticamaraBelum ada peringkat
- Burns Assessment and ManagementDokumen33 halamanBurns Assessment and ManagementErina Erichan Oto100% (1)
- BSBHRM506 Assessment 1Dokumen9 halamanBSBHRM506 Assessment 1prasannareddy9989Belum ada peringkat
- Filipino BrillianceDokumen6 halamanFilipino BrillianceEnerio EbisaBelum ada peringkat
- Professional Adjustment in NursingDokumen47 halamanProfessional Adjustment in NursingAnning HagarBelum ada peringkat
- Spanish ACLS Provider Manual ErrataDokumen2 halamanSpanish ACLS Provider Manual ErrataurbanincultureBelum ada peringkat
- Bacteriological Risk Analysis of Rural Water Supply Schemes in Western Development Region of NepalDokumen5 halamanBacteriological Risk Analysis of Rural Water Supply Schemes in Western Development Region of NepalmadhavBelum ada peringkat
- Health and Safety CultureDokumen2 halamanHealth and Safety CultureAbdul WahabBelum ada peringkat
- Talkshow #5Dokumen11 halamanTalkshow #540Thiên TrangB2Belum ada peringkat
- Exercise CH 04Dokumen9 halamanExercise CH 04Nurshuhada Nordin0% (1)
- Nursing Care Plan The Child or Adolescent Hospitalized With DepressionDokumen2 halamanNursing Care Plan The Child or Adolescent Hospitalized With DepressionVette Angelikka Dela CruzBelum ada peringkat
- Comorbid Drug Use Disorders and Eating Disorders - A Review of Prevalence StudiesDokumen12 halamanComorbid Drug Use Disorders and Eating Disorders - A Review of Prevalence StudiesJhon QuinteroBelum ada peringkat
- DORC HSE Department Contractors' Safety MeetingDokumen63 halamanDORC HSE Department Contractors' Safety MeetingJosiahBelum ada peringkat
- Levels of Professionalism Among Physical Therapists in India A National Cross Sectional Survey 2161 0673.1000123Dokumen6 halamanLevels of Professionalism Among Physical Therapists in India A National Cross Sectional Survey 2161 0673.1000123riddhiBelum ada peringkat