Anda mungkin juga menyukai
- Goljan Lectures Notes Part 1Dokumen317 halamanGoljan Lectures Notes Part 1walmarie0195% (19)
- Bio Cbse 12 Project On Hiv AisDokumen15 halamanBio Cbse 12 Project On Hiv Aishelo helium50% (2)
- Immunity QP New Syllabus (2010-2012)Dokumen40 halamanImmunity QP New Syllabus (2010-2012)Ae Banpong100% (1)
- Pedia MCUDokumen65 halamanPedia MCUfilchibuffBelum ada peringkat
- Benign Neoplasms of the Vulva, Vagina, Cervix and UterusDokumen11 halamanBenign Neoplasms of the Vulva, Vagina, Cervix and UterusIrene FranzBelum ada peringkat
- HepatitisDokumen20 halamanHepatitishnndisfh100% (1)
- First Aid LeafletDokumen11 halamanFirst Aid LeafletshahnawazBelum ada peringkat
- Odessa National Medical University: Surgical InfectionsDokumen34 halamanOdessa National Medical University: Surgical InfectionsDrRajneesh ShastriBelum ada peringkat
- Upper Respiratory Tract InfectionDokumen31 halamanUpper Respiratory Tract InfectionMASII100% (2)
- Dams Lastlook Microbiology PDFDokumen27 halamanDams Lastlook Microbiology PDFChauhan Monika100% (1)
- Lane J 1953 - Neotropical Culicidae Vol IDokumen550 halamanLane J 1953 - Neotropical Culicidae Vol IDavid Schiemann100% (3)
- Immunology Cell Biology - 2007 - Saunders - Life and Death in The Granuloma Immunopathology of TuberculosisDokumen9 halamanImmunology Cell Biology - 2007 - Saunders - Life and Death in The Granuloma Immunopathology of TuberculosisLily SmithBelum ada peringkat
- Sepsis and Septic ShockDokumen28 halamanSepsis and Septic ShockHayk MinasyanBelum ada peringkat
- Life and Death in The Granuloma: Immunopathology of TuberculosisDokumen9 halamanLife and Death in The Granuloma: Immunopathology of TuberculosisedelinBelum ada peringkat
- Clinical Evidence and Therapeutic Treatments at The Time of The Coronaviruses Responsible For SARS: A Perspective Point of ViewDokumen7 halamanClinical Evidence and Therapeutic Treatments at The Time of The Coronaviruses Responsible For SARS: A Perspective Point of ViewLorena SusatoBelum ada peringkat
- Mascelli NoDokumen10 halamanMascelli NoAung SoeBelum ada peringkat
- Cytokine Storm in COVID-19_ The Current Evidence and Treatment StrategiesDokumen33 halamanCytokine Storm in COVID-19_ The Current Evidence and Treatment StrategiesFitriBelum ada peringkat
- T Lymphocyte Exhaustion During Human and Experimental Visceral LeishmaniasisDokumen15 halamanT Lymphocyte Exhaustion During Human and Experimental Visceral LeishmaniasisLuis Carlos Calvanapon TerronesBelum ada peringkat
- Inflammation Seminar OverviewDokumen19 halamanInflammation Seminar OverviewDrGurinder Kanwar100% (1)
- Neutrophil in Chronic InflammationDokumen15 halamanNeutrophil in Chronic InflammationRizqaFebrilianyBelum ada peringkat
- Malaria Immunology 71Dokumen7 halamanMalaria Immunology 71Firda DamiruBelum ada peringkat
- Chlamydia Trachomatis Inhibits Apoptosis in Infected Cells by Targeting The Pro-Apoptotic Proteins Bax and BakDokumen14 halamanChlamydia Trachomatis Inhibits Apoptosis in Infected Cells by Targeting The Pro-Apoptotic Proteins Bax and BakJuan manuel jiménez estradaBelum ada peringkat
- Suptipos de SepsisDokumen17 halamanSuptipos de SepsisoswaldoninaBelum ada peringkat
- J Immunol 2005 Bagavant 944 50Dokumen8 halamanJ Immunol 2005 Bagavant 944 50Saad MotawéaBelum ada peringkat
- Pathogenesis of Inflammation: The Five Signs and MediatorsDokumen97 halamanPathogenesis of Inflammation: The Five Signs and MediatorsErutanature_Gr_9428Belum ada peringkat
- Infeksi StreptoDokumen6 halamanInfeksi StreptoRiris SutrisnoBelum ada peringkat
- 011 Management of Scrub PDFDokumen10 halaman011 Management of Scrub PDFNishmita NarayanBelum ada peringkat
- Cryptococcal Lung MycosesDokumen14 halamanCryptococcal Lung MycosesFebri Dwi HaryonoBelum ada peringkat
- Tropicalmed 07 00129Dokumen9 halamanTropicalmed 07 00129Colo VoltaBelum ada peringkat
- COVID-19 Physiopathology: EditorialDokumen3 halamanCOVID-19 Physiopathology: EditorialSOMMER ALONDRA BANDA MAMANIBelum ada peringkat
- Persistencia de ClamidyaDokumen13 halamanPersistencia de ClamidyaAnonymous tBJwSUSjBelum ada peringkat
- Delayed-Type Hypersensitivity and Granuloma FormationDokumen2 halamanDelayed-Type Hypersensitivity and Granuloma FormationDavid Saguil100% (1)
- Patofisiologi Malaria PDFDokumen11 halamanPatofisiologi Malaria PDFMeylinda LinBelum ada peringkat
- 7ads4663 74663 IJPapprovedDokumen13 halaman7ads4663 74663 IJPapprovedIndra HedarBelum ada peringkat
- COVID-19 A Recommendation To ExamineDokumen4 halamanCOVID-19 A Recommendation To ExamineDayalisis E. RodriguezBelum ada peringkat
- Pathophysiology of Malaria: How Parasite Infection Affects the BodyDokumen20 halamanPathophysiology of Malaria: How Parasite Infection Affects the Bodymelia100% (1)
- COVID-19: A Recommendation To Examine The Effect of Hydroxychloroquine in Preventing Infection and ProgressionDokumen4 halamanCOVID-19: A Recommendation To Examine The Effect of Hydroxychloroquine in Preventing Infection and ProgressionDaniel ChávezBelum ada peringkat
- Host Immune Response To Chlamydia InfectionDokumen17 halamanHost Immune Response To Chlamydia Infectionapi-266835840Belum ada peringkat
- Update On Psoriasis Immunopathogenesis and Targeted ImmunotherapyDokumen17 halamanUpdate On Psoriasis Immunopathogenesis and Targeted ImmunotherapyDevi Christina Damanik (Papua medical School)Belum ada peringkat
- Fat StudyDokumen79 halamanFat Studythe kingfishBelum ada peringkat
- jcm-10-00877 InvestigaçãoDokumen33 halamanjcm-10-00877 InvestigaçãoLucas Monteiro LopesBelum ada peringkat
- SirsDokumen29 halamanSirsfatimaBelum ada peringkat
- Neisseria MeningitidisDokumen3 halamanNeisseria MeningitidishedstrongBelum ada peringkat
- Cryptococcosis Pathogen Causes Deadly Fungal InfectionDokumen2 halamanCryptococcosis Pathogen Causes Deadly Fungal InfectionMaisarah SalsabilBelum ada peringkat
- Pathology1 PDFDokumen38 halamanPathology1 PDFAshes GhosalBelum ada peringkat
- Patogenesis Infeksi Bakteri, Infeksi Lokal, Dan SepsisDokumen52 halamanPatogenesis Infeksi Bakteri, Infeksi Lokal, Dan SepsisNia AnestyaBelum ada peringkat
- Clinical and Molecular Aspects of Vitiligo TreatmentsDokumen15 halamanClinical and Molecular Aspects of Vitiligo TreatmentsSabariaBelum ada peringkat
- General Pathology Key ConceptsDokumen16 halamanGeneral Pathology Key ConceptsSadii KhanBelum ada peringkat
- Inflammation: Inflammation Is A Protective Response, The Goal of Which Is To EliminateDokumen26 halamanInflammation: Inflammation Is A Protective Response, The Goal of Which Is To EliminateDavid Cahyo WibisonoBelum ada peringkat
- Cryoglobulinemia ReviewDokumen7 halamanCryoglobulinemia ReviewJosé Manuel Valencia GallardoBelum ada peringkat
- Syphilis: Using Modern Approaches To Understand An Old DiseaseDokumen9 halamanSyphilis: Using Modern Approaches To Understand An Old DiseaseAwalliantoniBelum ada peringkat
- Understanding an Old Disease Using Modern TechniquesDokumen9 halamanUnderstanding an Old Disease Using Modern TechniquesSteven LeonardoBelum ada peringkat
- 2007, Vol.25, Issues 4, Cutaneous Receptors - Clinical Implications and Therapeutic RelevanceDokumen202 halaman2007, Vol.25, Issues 4, Cutaneous Receptors - Clinical Implications and Therapeutic RelevanceRizweta DestinBelum ada peringkat
- Functional and Phenotypic Changes in Monocytes From Patients With Tuberculosis Are Reversed With TreatmentDokumen9 halamanFunctional and Phenotypic Changes in Monocytes From Patients With Tuberculosis Are Reversed With TreatmentCecile E EcheverríaBelum ada peringkat
- Interplay Between Alveolar Epithelial and Dendritic Cells andDokumen18 halamanInterplay Between Alveolar Epithelial and Dendritic Cells andTamara RodriguesBelum ada peringkat
- Elife 77345 v1Dokumen48 halamanElife 77345 v1Afandi CharlesBelum ada peringkat
- Cutaneous Lupus Erythematosus: A Review of Pathogenesis, Presentation, Diagnosis and TreatmentDokumen198 halamanCutaneous Lupus Erythematosus: A Review of Pathogenesis, Presentation, Diagnosis and TreatmentRizweta DestinBelum ada peringkat
- Articulo Obesidad Covid-19Dokumen10 halamanArticulo Obesidad Covid-19Victor Hugo CurasiBelum ada peringkat
- Br. J. Anaesth. 2012 Reid Bja Aes321Dokumen11 halamanBr. J. Anaesth. 2012 Reid Bja Aes321Maria RomeroBelum ada peringkat
- Sem1P1 (41-60)Dokumen19 halamanSem1P1 (41-60)Thom TimkangBelum ada peringkat
- Fall_Metabolomics_accepted_versionDokumen37 halamanFall_Metabolomics_accepted_versionmichel.aug.silvaBelum ada peringkat
- Cell Deaths - Involvement in The Pathogenesis and InterventionDokumen21 halamanCell Deaths - Involvement in The Pathogenesis and InterventionSHREYA SENTHIL KUMAR IMS21286Belum ada peringkat
- Psoriasis pathophysiology current conceptsofpathogenesisDokumen7 halamanPsoriasis pathophysiology current conceptsofpathogenesisAnnaBelum ada peringkat
- AIDSDokumen32 halamanAIDSJuwairia tariqBelum ada peringkat
- Disorders of Granulocytes and MonocytesDokumen45 halamanDisorders of Granulocytes and Monocytesswathi bsBelum ada peringkat
- Path4 5aDokumen89 halamanPath4 5aAbid KhanBelum ada peringkat
- Review of Toxic Epidermal NecrolysisDokumen10 halamanReview of Toxic Epidermal NecrolysisNurfitri ZuhruhurBelum ada peringkat
- Cytomegalovirus InfectionDokumen18 halamanCytomegalovirus InfectionpuaanBelum ada peringkat
- Histamine Antagonists To Temper The Cytokine Overproduction in Gastrointestinal Cells Infected by Sars-Cov-2Dokumen15 halamanHistamine Antagonists To Temper The Cytokine Overproduction in Gastrointestinal Cells Infected by Sars-Cov-2MichaelBelum ada peringkat
- Poster FormatDokumen1 halamanPoster Formataldea_844577109Belum ada peringkat
- Propunere Alyssa Events - CompressedDokumen40 halamanPropunere Alyssa Events - Compressedaldea_844577109Belum ada peringkat
- COVID-19 Algorithm5 PDFDokumen1 halamanCOVID-19 Algorithm5 PDFSofia Tous DeBelum ada peringkat
- Epigenetics: Intrauterine Growth Retardation (IUGR) Modifies The Histone Code Along The Rat Hepatic IGF-1 GeneDokumen12 halamanEpigenetics: Intrauterine Growth Retardation (IUGR) Modifies The Histone Code Along The Rat Hepatic IGF-1 Genealdea_844577109Belum ada peringkat
- Peter Duerre - Handbook On Clostridia-CRC Press (2004) PDFDokumen1.156 halamanPeter Duerre - Handbook On Clostridia-CRC Press (2004) PDFaldea_844577109100% (1)
- AbbreviationDokumen1 halamanAbbreviationaldea_844577109Belum ada peringkat
- Tabel Infection After MIADokumen2 halamanTabel Infection After MIAaldea_844577109Belum ada peringkat
- C.Sordellii Contamination: Phagocytes in Endometrium Proinflamatory Cytokines Release Weaken Innate Immune SystemDokumen1 halamanC.Sordellii Contamination: Phagocytes in Endometrium Proinflamatory Cytokines Release Weaken Innate Immune Systemaldea_844577109Belum ada peringkat
- AbbreviationDokumen1 halamanAbbreviationaldea_844577109Belum ada peringkat
- C.Sordellii Contamination: Phagocytes in Endometrium Proinflamatory Cytokines Release Weaken Innate Immune SystemDokumen1 halamanC.Sordellii Contamination: Phagocytes in Endometrium Proinflamatory Cytokines Release Weaken Innate Immune Systemaldea_844577109Belum ada peringkat
- Fetal and placental size linked to adult hypertension riskDokumen4 halamanFetal and placental size linked to adult hypertension riskaldea_844577109Belum ada peringkat
- Pag 2Dokumen5 halamanPag 2Claume70Belum ada peringkat
- Principle: Identification System For Staphylococci and MicrococciDokumen8 halamanPrinciple: Identification System For Staphylococci and MicrococciVictor PABelum ada peringkat
- Covid 19 PDFDokumen117 halamanCovid 19 PDFvicky anandBelum ada peringkat
- Isolation of Pathogens Causing Sepsis Pus and Infected Wounds From Critical Care Unit A Retrospective Study - 2Dokumen8 halamanIsolation of Pathogens Causing Sepsis Pus and Infected Wounds From Critical Care Unit A Retrospective Study - 2Omoding EmmanuelBelum ada peringkat
- Wanted Microorganism Poster Activity RubricDokumen3 halamanWanted Microorganism Poster Activity Rubricapi-454028760Belum ada peringkat
- Thomson - The Excretory SystemDokumen24 halamanThomson - The Excretory Systemapi-263178717Belum ada peringkat
- Parvo BacteriaDokumen2 halamanParvo BacteriaErnie G. Bautista II, RN, MDBelum ada peringkat
- A MatrixDokumen11 halamanA MatrixChristian MakandeBelum ada peringkat
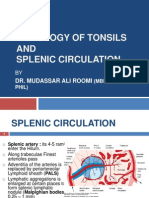
- Histology of Tonsil and Splenic Circulation by Dr. RoomiDokumen21 halamanHistology of Tonsil and Splenic Circulation by Dr. RoomiMudassar RoomiBelum ada peringkat
- Essential Biology Unit 18Dokumen4 halamanEssential Biology Unit 18Poornima AthikariBelum ada peringkat
- Pathophysiology of Viral GastroenteritisDokumen2 halamanPathophysiology of Viral GastroenteritisJun MingBelum ada peringkat
- Infection ControlDokumen235 halamanInfection Controldisaster6993Belum ada peringkat
- FAMILY PLanning FinalDokumen23 halamanFAMILY PLanning FinalLebo Ramokolo100% (1)
- Homeostatic Imbalances: in The Integumentary SystemDokumen27 halamanHomeostatic Imbalances: in The Integumentary SystemMarilou Dacles IIBelum ada peringkat
- B.ph.-3 Yr Cognosy Unit 4 As Per Ruhs 2014Dokumen53 halamanB.ph.-3 Yr Cognosy Unit 4 As Per Ruhs 2014Pankaj DhootBelum ada peringkat
- Brief History of EpidemiologyDokumen9 halamanBrief History of EpidemiologyLuningning UmarBelum ada peringkat
- BibliographyDokumen11 halamanBibliographyapi-124468116Belum ada peringkat
- Philippine high school exam on Southeast Asian culture and musicDokumen3 halamanPhilippine high school exam on Southeast Asian culture and musicjanice m. gasparBelum ada peringkat
- TranspositionDokumen21 halamanTranspositionponderofbiotechBelum ada peringkat
- Plaque: Dr. Marcel Rene C. HallareDokumen17 halamanPlaque: Dr. Marcel Rene C. Hallareceudmd3dBelum ada peringkat