Anda mungkin juga menyukai
- 80DDDokumen1 halaman80DDranjithpatel.ttidBelum ada peringkat
- Form 10IADokumen1 halamanForm 10IAkktbrr1Belum ada peringkat
- Form 10IADokumen1 halamanForm 10IAshailendra parmarBelum ada peringkat
- Form 10IADokumen1 halamanForm 10IAmanickam.ramlakshBelum ada peringkat
- Formno.10 IaDokumen1 halamanFormno.10 IajsparakhBelum ada peringkat
- 800 DDBDokumen1 halaman800 DDBguru prasathBelum ada peringkat
- Form 10IADokumen1 halamanForm 10IAkktbrr1Belum ada peringkat
- Form No 10-IaDokumen1 halamanForm No 10-Iacooldude32166Belum ada peringkat
- Form No 10-IaDokumen1 halamanForm No 10-IaMd Waseem KBelum ada peringkat
- Form 10 IADokumen1 halamanForm 10 IASomesubhra DasBelum ada peringkat
- FINAL CAT-III ADVT (2022) Final - 39-42Dokumen4 halamanFINAL CAT-III ADVT (2022) Final - 39-42jackBelum ada peringkat
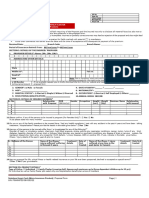
- Disability Certificate Form - I: Recent PP Size Attested Photograph (Showing Face Only) of The Person With DisabilityDokumen6 halamanDisability Certificate Form - I: Recent PP Size Attested Photograph (Showing Face Only) of The Person With DisabilityHemant KumarBelum ada peringkat
- (Name and Address of The Medical Authority Issuing The Certificate) (See Rule 4)Dokumen2 halaman(Name and Address of The Medical Authority Issuing The Certificate) (See Rule 4)Saurav SharmaBelum ada peringkat
- EWS PWD OBC Certificate FormatsDokumen5 halamanEWS PWD OBC Certificate FormatsbiztigerrBelum ada peringkat
- Certificate For The Persons With DisabilitiesDokumen1 halamanCertificate For The Persons With DisabilitiesDebajit MalakarBelum ada peringkat
- Disablity Certificate FormatDokumen2 halamanDisablity Certificate FormatSudeshana JainBelum ada peringkat
- MBA Admission 2024 AnnexureDokumen2 halamanMBA Admission 2024 AnnexurePrem DhivakarBelum ada peringkat
- GRANTDokumen3 halamanGRANTrojith rojithBelum ada peringkat
- Income Certificate Formats For JosaaDokumen9 halamanIncome Certificate Formats For JosaaAnirban GhoshBelum ada peringkat
- Disability Certificate (PWD) Form VI 2022Dokumen2 halamanDisability Certificate (PWD) Form VI 2022blogwriter048Belum ada peringkat
- Authorised Third Party Representative FormDokumen6 halamanAuthorised Third Party Representative FormJimBelum ada peringkat
- Health Declaration FormDokumen1 halamanHealth Declaration FormCalleja Jemimah Rose AristokiBelum ada peringkat
- Useful TipsDokumen2 halamanUseful Tipschaudhary.sunil22Belum ada peringkat
- DL-13 Medicall Reporting Form To Request Removal of Driving PrivDokumen1 halamanDL-13 Medicall Reporting Form To Request Removal of Driving PrivPA Work LicenseBelum ada peringkat
- THDC India Limited: From D' Life CertificateDokumen1 halamanTHDC India Limited: From D' Life CertificateTHDC OFFICERS CLUBBelum ada peringkat
- Circular No. 2020-010Dokumen8 halamanCircular No. 2020-010Mercado MartinBelum ada peringkat
- Claim Benefirs Checklist Ci2020-010Dokumen8 halamanClaim Benefirs Checklist Ci2020-010Aljohn SebucBelum ada peringkat
- PMDC Form IVDokumen5 halamanPMDC Form IVRaza Ze0% (1)
- (176736967) PMRF - RevisedDokumen3 halaman(176736967) PMRF - Revisedanon_902897556Belum ada peringkat
- Certificate of Disability Form-VI PDFDokumen3 halamanCertificate of Disability Form-VI PDFpyro_pradeepBelum ada peringkat
- FileHandler PDFDokumen2 halamanFileHandler PDFRoman ReignsBelum ada peringkat
- IMMI Grant NotificationDokumen3 halamanIMMI Grant NotificationJagdhara KarthiBelum ada peringkat
- Disability (4long) - 03102014-Adr PDFDokumen4 halamanDisability (4long) - 03102014-Adr PDFGianJyrellAlbertoCorletBelum ada peringkat
- Dr. B. R. Ambedkar National Law University, Rai, Sonipat: (In Capital Letters)Dokumen3 halamanDr. B. R. Ambedkar National Law University, Rai, Sonipat: (In Capital Letters)Sona NarulaBelum ada peringkat
- Bahagian 1: Maklumat Sijil: Nomination FormDokumen2 halamanBahagian 1: Maklumat Sijil: Nomination FormawanBelum ada peringkat
- De2501fc 2Dokumen4 halamanDe2501fc 2PayPal PlcBelum ada peringkat
- Medical Reimbursemen APPLICATION SETDokumen5 halamanMedical Reimbursemen APPLICATION SETLeelakrishna GvBelum ada peringkat
- PhilHealth Member Registration Form (PMRF)Dokumen2 halamanPhilHealth Member Registration Form (PMRF)Vinson Gabato78% (9)
- AbndgjdksvdkkdjDokumen4 halamanAbndgjdksvdkkdjEn KayBelum ada peringkat
- #Nem Check List Rakyat Individual - Che Samsiah 4.23kwpDokumen24 halaman#Nem Check List Rakyat Individual - Che Samsiah 4.23kwphafezzbusraBelum ada peringkat
- Transaction Details: Product Type Loan Amount/Premium (RS.) Downpayment (RS.) EMI Amount (RS.)Dokumen3 halamanTransaction Details: Product Type Loan Amount/Premium (RS.) Downpayment (RS.) EMI Amount (RS.)Seela VaraprasadBelum ada peringkat
- IMMI Grant NotificationDokumen3 halamanIMMI Grant Notificationpaula ocampo100% (1)
- Driver Medical Examination Report Form TemplateDokumen9 halamanDriver Medical Examination Report Form TemplateMIkeBelum ada peringkat
- DataFlow Application PackDokumen8 halamanDataFlow Application PackMichelle TolentinoBelum ada peringkat
- Sukshma Hospi CashDokumen4 halamanSukshma Hospi CashAdemuyiwa OlaniyiBelum ada peringkat
- Paramount Health Services & Insurance Tpa Private Limited: First Reminder Letter Without PrejudiceDokumen1 halamanParamount Health Services & Insurance Tpa Private Limited: First Reminder Letter Without PrejudiceTanmoy Pal ChowdhuryBelum ada peringkat
- HandicapDokumen2 halamanHandicapdvolmy321Belum ada peringkat
- Letter of Authorization: Personal DetailsDokumen1 halamanLetter of Authorization: Personal DetailsMrunal DoiphodeBelum ada peringkat
- Exit From National Pension System Due To Premature ExitDokumen6 halamanExit From National Pension System Due To Premature ExitPUNAM RNDBelum ada peringkat
- Haryana Provisional RegistrationDokumen5 halamanHaryana Provisional RegistrationAMARBelum ada peringkat
- Manual Policy Owner's Manual Policy Owner's Manual: Individual Underwriting FormDokumen2 halamanManual Policy Owner's Manual Policy Owner's Manual: Individual Underwriting FormankurBelum ada peringkat
- Aia Takaful Hopitalisation Claim FormDokumen4 halamanAia Takaful Hopitalisation Claim Formmohd rashidiBelum ada peringkat
- Overseas Travel Insurance Claim FormDokumen3 halamanOverseas Travel Insurance Claim FormSumit BhandariBelum ada peringkat
- Cross-Training: The Medical Assistant WorkbookDari EverandCross-Training: The Medical Assistant WorkbookBelum ada peringkat
- Everything You Always Wanted to Know About Social Security Disability LawDari EverandEverything You Always Wanted to Know About Social Security Disability LawBelum ada peringkat
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsDari EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsBelum ada peringkat