Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Self-Assessment Questions Chapter 8 The Urinary SystemDokumen10 halamanSelf-Assessment Questions Chapter 8 The Urinary Systemsanam shahzadi100% (1)
- FNP 3 - JiaDokumen16 halamanFNP 3 - Jiaapi-551073862100% (1)
- Comprehensive Critical Care UltrasoundDokumen692 halamanComprehensive Critical Care UltrasoundRonei Renato RubboBelum ada peringkat
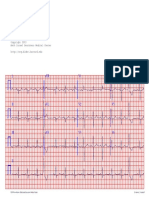
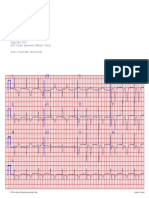
- EKG in IHDDokumen349 halamanEKG in IHDDinhLinh100% (1)
- Medical Emergencies in The Dental Office 6th Edition Malamed Test BankDokumen2 halamanMedical Emergencies in The Dental Office 6th Edition Malamed Test BankKieranPenaBelum ada peringkat
- Carol Davila Pathophysiology NotesDokumen7 halamanCarol Davila Pathophysiology NotesGiorgos Doukas KaranasiosBelum ada peringkat
- Caz 22 PDFDokumen1 halamanCaz 22 PDFIoana CozmaBelum ada peringkat
- Caz 83 PDFDokumen1 halamanCaz 83 PDFIoana CozmaBelum ada peringkat
- Caz 5 PDFDokumen1 halamanCaz 5 PDFIoana CozmaBelum ada peringkat
- Caz 11 PDFDokumen1 halamanCaz 11 PDFIoana CozmaBelum ada peringkat
- Caz 92 PDFDokumen1 halamanCaz 92 PDFIoana CozmaBelum ada peringkat
- Caz 12 PDFDokumen1 halamanCaz 12 PDFIoana CozmaBelum ada peringkat
- Complications PDFDokumen79 halamanComplications PDFIoana CozmaBelum ada peringkat
- Infectious Diseases. Etiology PDFDokumen76 halamanInfectious Diseases. Etiology PDFIoana CozmaBelum ada peringkat
- Caz 53 PDFDokumen1 halamanCaz 53 PDFIoana CozmaBelum ada peringkat
- 03 - Thorax 2 PDFDokumen93 halaman03 - Thorax 2 PDFIoana CozmaBelum ada peringkat
- Caz 17 PDFDokumen1 halamanCaz 17 PDFIoana CozmaBelum ada peringkat
- Caz 14 PDFDokumen1 halamanCaz 14 PDFIoana CozmaBelum ada peringkat
- Caz 22 PDFDokumen1 halamanCaz 22 PDFIoana CozmaBelum ada peringkat
- Caz 13 PDFDokumen1 halamanCaz 13 PDFIoana CozmaBelum ada peringkat
- ATA Guidelines for Management of Differentiated Thyroid CancerDokumen28 halamanATA Guidelines for Management of Differentiated Thyroid CancerIoana CozmaBelum ada peringkat
- Caz 240 PDFDokumen1 halamanCaz 240 PDFIoana CozmaBelum ada peringkat
- Introduction PDFDokumen21 halamanIntroduction PDFIoana CozmaBelum ada peringkat
- LEC 03 - Pituitary TumoursDokumen54 halamanLEC 03 - Pituitary TumoursIoana CozmaBelum ada peringkat
- General Survey (Lecture 1)Dokumen91 halamanGeneral Survey (Lecture 1)Ioana CozmaBelum ada peringkat
- Definitions PDFDokumen7 halamanDefinitions PDFIoana CozmaBelum ada peringkat
- LEC 01 - Principles of EndocrinologyDokumen44 halamanLEC 01 - Principles of EndocrinologyIoana Cozma100% (1)
- LEC 04 - Hypo - Hyperthyroidism PDFDokumen115 halamanLEC 04 - Hypo - Hyperthyroidism PDFIoana CozmaBelum ada peringkat
- CHD Engl Nou!!Dokumen96 halamanCHD Engl Nou!!Ioana CozmaBelum ada peringkat
- LEC 04 - Hypo - Hyperthyroidism PDFDokumen115 halamanLEC 04 - Hypo - Hyperthyroidism PDFIoana CozmaBelum ada peringkat
- LEC 05 - Growth - Puberty DisordersDokumen58 halamanLEC 05 - Growth - Puberty DisordersIoana CozmaBelum ada peringkat
- Pituitary Tumor Types, Causes, and TreatmentsDokumen54 halamanPituitary Tumor Types, Causes, and TreatmentsIoana CozmaBelum ada peringkat
- Lecture 2B - Fetal Presentations and Positions During DeliveryDokumen40 halamanLecture 2B - Fetal Presentations and Positions During DeliveryIoana CozmaBelum ada peringkat
- LEC 02 - Hypothalamus - Hypopituitarism PDFDokumen31 halamanLEC 02 - Hypothalamus - Hypopituitarism PDFIoana CozmaBelum ada peringkat
- Genitourinary Infections GuideDokumen56 halamanGenitourinary Infections GuideIoana CozmaBelum ada peringkat
- New Mock 1-2022Dokumen29 halamanNew Mock 1-2022nemalijyothsna3Belum ada peringkat
- Mubeens Clinical Examinations Crib Sheet PDFDokumen36 halamanMubeens Clinical Examinations Crib Sheet PDFTimothy HarwichBelum ada peringkat
- Liver Cirrhosis and Neurological Disorder Associated With Liver DiseaseDokumen10 halamanLiver Cirrhosis and Neurological Disorder Associated With Liver DiseaseEditor IJTSRDBelum ada peringkat
- Hepatocellular Carcinoma and Other Hepatic MassesDokumen59 halamanHepatocellular Carcinoma and Other Hepatic MassesIsaac MwangiBelum ada peringkat
- The PAPP Pulmonary Care of Long COVID in ChildrenDokumen25 halamanThe PAPP Pulmonary Care of Long COVID in ChildrenAC Vallester100% (1)
- Quick Reference Handbook: Guidelines For Crises in AnaesthesiaDokumen30 halamanQuick Reference Handbook: Guidelines For Crises in AnaesthesiaazeezBelum ada peringkat
- Biochem Uni QuestionsDokumen6 halamanBiochem Uni Questionsgrivapatel20092002Belum ada peringkat
- Clinical Manifestations and Complications of Inflammatory Bowel Disease in Children and Adolescents - UpToDateDokumen35 halamanClinical Manifestations and Complications of Inflammatory Bowel Disease in Children and Adolescents - UpToDateTurma A 2019.1 Med-FCMBelum ada peringkat
- Amboss - Thoracic CavityDokumen14 halamanAmboss - Thoracic CavityAllysahBelum ada peringkat
- Nclex Study Questions AcidDokumen5 halamanNclex Study Questions AcidTabatha LedbetterBelum ada peringkat
- Pharmacological Properties of Beta-Adrenoceptor Blocking DrugsDokumen6 halamanPharmacological Properties of Beta-Adrenoceptor Blocking DrugsProduct DepartementBelum ada peringkat
- Patient Case 1 2Dokumen3 halamanPatient Case 1 2Maria Lizzyree LutaoBelum ada peringkat
- Spinal Cord ExternalDokumen33 halamanSpinal Cord ExternalCosplay AccountBelum ada peringkat
- JurdingDokumen19 halamanJurdingifaans16Belum ada peringkat
- Cardiovascular Perfusion ThesisDokumen4 halamanCardiovascular Perfusion Thesisamandagraytulsa100% (2)
- Post Operative HypotensionDokumen7 halamanPost Operative HypotensionbbyesBelum ada peringkat
- BLOOD PRODUCT TRANSFUSIONS DEFINITIONS AND TRANSFUSION REACTIONSDokumen1 halamanBLOOD PRODUCT TRANSFUSIONS DEFINITIONS AND TRANSFUSION REACTIONSjuan ramon milanes grageraBelum ada peringkat
- 2015 ERASAnaesthesiaPart2 PDFDokumen47 halaman2015 ERASAnaesthesiaPart2 PDFAbhishek LonikarBelum ada peringkat
- Dorval 2009Dokumen9 halamanDorval 2009frcubidesBelum ada peringkat
- PiCCO TechologyDokumen24 halamanPiCCO Techology吳哲慰Belum ada peringkat
- Understanding the Cardiovascular SystemDokumen7 halamanUnderstanding the Cardiovascular SystemKhrean Kae SantiagoBelum ada peringkat
- Eosinophil Biology and Causes of Eosinophilia - UpToDateDokumen35 halamanEosinophil Biology and Causes of Eosinophilia - UpToDateBls PriyaBelum ada peringkat
- ECG For Beginners PDFDokumen153 halamanECG For Beginners PDFIonut MoisaBelum ada peringkat
- VitalsignsDokumen7 halamanVitalsignsSalazar, Lourish Ann G. BSN2-CBelum ada peringkat
- BNF drugs for asthma, infections and arrhythmiasDokumen2 halamanBNF drugs for asthma, infections and arrhythmiasgege0% (1)