Anda mungkin juga menyukai
- Qdoc - Tips - Astm d523 08 Standard Test Method For Specular GloDokumen5 halamanQdoc - Tips - Astm d523 08 Standard Test Method For Specular GlofaizBelum ada peringkat
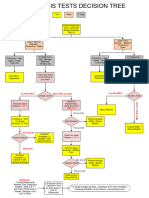
- Hypothesis Tests Decision TreeDokumen2 halamanHypothesis Tests Decision TreeD RagulBelum ada peringkat
- Chemical Equilibrium - Mind Map - Arjuna JEE 2024Dokumen1 halamanChemical Equilibrium - Mind Map - Arjuna JEE 2024neavjain2007Belum ada peringkat
- Atellica Solution CH Analyzer Assay Chart, 11484427 Rev 04, EN DXDCM 09017fe9807b250b-1676056852193Dokumen26 halamanAtellica Solution CH Analyzer Assay Chart, 11484427 Rev 04, EN DXDCM 09017fe9807b250b-1676056852193chinuswami100% (3)
- Code Blue Running SheetDokumen2 halamanCode Blue Running Sheetenumula kumar100% (12)
- Poston Scale Packet: Concert F MajorDokumen6 halamanPoston Scale Packet: Concert F MajoralxemnatalBelum ada peringkat
- Poston Scale Packet: Concert F MajorDokumen6 halamanPoston Scale Packet: Concert F Major권ᄒᄇᄒBelum ada peringkat
- Bassoon Scales PDFDokumen6 halamanBassoon Scales PDFeeeBelum ada peringkat
- Statistical FrameworkDokumen1 halamanStatistical FrameworksoraruBelum ada peringkat
- Graphpad Flowchart PDFDokumen1 halamanGraphpad Flowchart PDFfrrreshBelum ada peringkat
- Graphpad-Flowchart PDFDokumen1 halamanGraphpad-Flowchart PDFNerdy JoeBelum ada peringkat
- SCH4UDokumen2 halamanSCH4UHuang EmilyBelum ada peringkat
- Atellica IM Analyzer Assay Chart, 11314389 Rev03, EN DXDCM 09017fe980577c45-1621893892636Dokumen10 halamanAtellica IM Analyzer Assay Chart, 11314389 Rev03, EN DXDCM 09017fe980577c45-1621893892636chinuswami100% (1)
- S149 FlowchartDokumen1 halamanS149 FlowchartAirah Jean AbadBelum ada peringkat
- Mind MapDokumen1 halamanMind Mapangelica.amandy.gBelum ada peringkat
- Grade 10 Phil - Iri Miscues and FRDokumen4 halamanGrade 10 Phil - Iri Miscues and FRKerbyjo Magadan ToongBelum ada peringkat
- Pharmacodynamics - DRC, Agonist - AntagonistDokumen6 halamanPharmacodynamics - DRC, Agonist - AntagonistPriyam Kishore DuttaBelum ada peringkat
- IG2 Day 2 Element 5Dokumen8 halamanIG2 Day 2 Element 5Risvan UbaisBelum ada peringkat
- Epinephrine: Adrenergic ReceptorsDokumen12 halamanEpinephrine: Adrenergic ReceptorsRed StohlBelum ada peringkat
- Français Français: o o o o o o o oDokumen18 halamanFrançais Français: o o o o o o o oTakieddine BenlahcenBelum ada peringkat
- Adobe Scan 04 Jul 2023Dokumen4 halamanAdobe Scan 04 Jul 2023manas ranjan hotaBelum ada peringkat
- Mas-I Formula Sheet PDFDokumen7 halamanMas-I Formula Sheet PDFUngoliant101Belum ada peringkat
- 11313257VFT000-01 Centaur XP Assay ChartDokumen10 halaman11313257VFT000-01 Centaur XP Assay ChartMedo O. EzzatBelum ada peringkat
- Scales With ThridsDokumen6 halamanScales With ThridsPreston Byrd Wilkes100% (1)
- Physio Initial Assessment Form: Glasgow Coma ScaleDokumen1 halamanPhysio Initial Assessment Form: Glasgow Coma Scalechetha kundiBelum ada peringkat
- 2021 2022 Kinder Grading SheetDokumen9 halaman2021 2022 Kinder Grading Sheetlynore sandovalBelum ada peringkat
- Gibbs Adsorption Isotherm NotesDokumen3 halamanGibbs Adsorption Isotherm NotesAshish ChauhanBelum ada peringkat
- KOMET Study Levetiracetam Vs DepakineDokumen4 halamanKOMET Study Levetiracetam Vs DepakineveerrajuBelum ada peringkat
- D1102 84 (Reapproved 2013) Ash in WoodDokumen2 halamanD1102 84 (Reapproved 2013) Ash in WoodChoirun NisaBelum ada peringkat
- Lesson 5b Test BlueprintDokumen16 halamanLesson 5b Test Blueprintssskgu100% (6)
- Flow Chart For Singly Reinforced BeamsDokumen1 halamanFlow Chart For Singly Reinforced BeamsRekanBelum ada peringkat
- RUBRIC - Speech DemonstrationDokumen1 halamanRUBRIC - Speech DemonstrationYuGenBelum ada peringkat
- BLS AclsDokumen8 halamanBLS Aclsvmmakhania.91Belum ada peringkat
- CFA Level I SmartSheet 2020Dokumen9 halamanCFA Level I SmartSheet 2020yousefBelum ada peringkat
- Exam Table For Adult ReconDokumen7 halamanExam Table For Adult ReconLouie OkayBelum ada peringkat
- Kenya Artsbridge Peer EvaluationDokumen1 halamanKenya Artsbridge Peer Evaluationapi-313790994Belum ada peringkat
- Siemens Healthcare Diagnostics Inc.: ADVIA Centaur XP Version 1.0.EC and 1.0.ED Test DefinitionsDokumen12 halamanSiemens Healthcare Diagnostics Inc.: ADVIA Centaur XP Version 1.0.EC and 1.0.ED Test DefinitionsОлександрBelum ada peringkat
- Apgar Score Description PDFDokumen1 halamanApgar Score Description PDFAira Shane MargesBelum ada peringkat
- Poster Chapter 2.2 & 3Dokumen1 halamanPoster Chapter 2.2 & 3Riyad RahmanBelum ada peringkat
- Pregnancy Info Sheet SBM PDFDokumen2 halamanPregnancy Info Sheet SBM PDFRameesa KhanBelum ada peringkat
- Beed 3a Building BridgesDokumen8 halamanBeed 3a Building BridgesMaricris Galman SalamatBelum ada peringkat
- 1.-Correlational-Analysis-1-of-2 3Dokumen1 halaman1.-Correlational-Analysis-1-of-2 3Precious Jewel EstoestaBelum ada peringkat
- Analisis Item Bi Paper 1Dokumen12 halamanAnalisis Item Bi Paper 1Muhamad Zulhaizad AmranBelum ada peringkat
- Homeostasis Concept MapDokumen1 halamanHomeostasis Concept MapMarjorie RonquilloBelum ada peringkat
- Vozoff 1972 Geophysics PDFDokumen44 halamanVozoff 1972 Geophysics PDFWilhelmBerrocalBelum ada peringkat
- Infographic Humanistic PsychologyDokumen2 halamanInfographic Humanistic Psychologyvivain.honnalli.officialBelum ada peringkat
- Hydro Test JSADokumen4 halamanHydro Test JSArk3050037Belum ada peringkat
- CNS: Headach E, Dizzines S, Vertigo, Nerve Root Lesion, Asthenia, InsomniDokumen8 halamanCNS: Headach E, Dizzines S, Vertigo, Nerve Root Lesion, Asthenia, InsomniHsintan HsuBelum ada peringkat
- Uji Univariat: Frequency TableDokumen6 halamanUji Univariat: Frequency TableAndrian novika sariBelum ada peringkat
- Uji Univariat: Frequency TableDokumen6 halamanUji Univariat: Frequency TableAndrian novika sariBelum ada peringkat
- PARTOGRAPHDokumen2 halamanPARTOGRAPHZairah Mae BangguiyaoBelum ada peringkat
- Materials 13 03396 v2Dokumen15 halamanMaterials 13 03396 v2ratinonphuBelum ada peringkat
- 2015 Instructor Manual - English Metric1Dokumen252 halaman2015 Instructor Manual - English Metric1DidosakBelum ada peringkat
- Knowledge Network of DSP Articles On WikipediaDokumen1 halamanKnowledge Network of DSP Articles On WikipediaHuJayBelum ada peringkat
- Hons I Student Monthly ReportDokumen2 halamanHons I Student Monthly ReportArpita SoniBelum ada peringkat
- Physics-Prashant Jaiswal Chemistry - Wassim Ahmad Bhat Biology - Sunil Bhaidasn A, Dinesh TalrejaDokumen7 halamanPhysics-Prashant Jaiswal Chemistry - Wassim Ahmad Bhat Biology - Sunil Bhaidasn A, Dinesh Talreja04 Dhairya PatelBelum ada peringkat
- Tubeless Percutaneous Nephrolithotomy: Spinal Versus General AnesthesiaDokumen5 halamanTubeless Percutaneous Nephrolithotomy: Spinal Versus General AnesthesiaDella Puspita SariBelum ada peringkat
- 4291 20312 2 PBDokumen5 halaman4291 20312 2 PBDella Puspita SariBelum ada peringkat
- Free PPT Templates: Insert The Sub Title of Your PresentationDokumen48 halamanFree PPT Templates: Insert The Sub Title of Your PresentationDella Puspita SariBelum ada peringkat
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDokumen5 halamanSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariBelum ada peringkat
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDokumen5 halamanSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariBelum ada peringkat
- Results and Complications of Spinal Anesthesia in Percutaneous NephrolithotomyDokumen4 halamanResults and Complications of Spinal Anesthesia in Percutaneous NephrolithotomyDella Puspita SariBelum ada peringkat
- Stetoskop PresentDokumen34 halamanStetoskop PresentSam 6928Belum ada peringkat
- 4291 20312 2 PBDokumen5 halaman4291 20312 2 PBDella Puspita SariBelum ada peringkat
- Results and Complications of Spinal Anesthesia in Percutaneous NephrolithotomyDokumen4 halamanResults and Complications of Spinal Anesthesia in Percutaneous NephrolithotomyDella Puspita SariBelum ada peringkat
- Wiedeman Comparison of Two Fluid-Management Strategies in Acute Lung Injury NEJM 2006Dokumen12 halamanWiedeman Comparison of Two Fluid-Management Strategies in Acute Lung Injury NEJM 2006Della Puspita SariBelum ada peringkat
- Tubeless Percutaneous Nephrolithotomy: Spinal Versus General AnesthesiaDokumen5 halamanTubeless Percutaneous Nephrolithotomy: Spinal Versus General AnesthesiaDella Puspita SariBelum ada peringkat
- Fibrion-Tetagam DXMDokumen33 halamanFibrion-Tetagam DXMDella Puspita SariBelum ada peringkat
- Survival Analysis Using SPSSDokumen57 halamanSurvival Analysis Using SPSSulisessaldiasroaBelum ada peringkat
- Cetin 2016Dokumen10 halamanCetin 2016Della Puspita SariBelum ada peringkat
- The Surgical Outcome of Total Urogenital Mobilization For Cloacal RepairDokumen4 halamanThe Surgical Outcome of Total Urogenital Mobilization For Cloacal RepairDella Puspita SariBelum ada peringkat
- Fibrion-Tetagam DXMDokumen33 halamanFibrion-Tetagam DXMDella Puspita SariBelum ada peringkat
- Analysis of Y Chromosome Microdeletion in Indonesian MalesDokumen7 halamanAnalysis of Y Chromosome Microdeletion in Indonesian MalesDella Puspita SariBelum ada peringkat
- Commentary: Digoxin in Chronic Heart Failure: Possibility of A Second Chance?Dokumen3 halamanCommentary: Digoxin in Chronic Heart Failure: Possibility of A Second Chance?Della Puspita SariBelum ada peringkat
- Arterioscler Thromb Vasc Biol 2002 Rosendaal 201 10Dokumen11 halamanArterioscler Thromb Vasc Biol 2002 Rosendaal 201 10Della Puspita SariBelum ada peringkat
- Hamza 2001Dokumen3 halamanHamza 2001Della Puspita SariBelum ada peringkat
- Screenshot Pencarian Digoxin ElderlyDokumen2 halamanScreenshot Pencarian Digoxin ElderlyDella Puspita SariBelum ada peringkat
- Wesam R KadhumDokumen31 halamanWesam R Kadhumwisam_1by1Belum ada peringkat
- BP502TP Papers of Sem 5Dokumen2 halamanBP502TP Papers of Sem 5KavanBelum ada peringkat
- Hesi RN Exit Exam V3Dokumen37 halamanHesi RN Exit Exam V3Eniti100% (1)
- Care of Patients With Acute Biologic CrisisDokumen72 halamanCare of Patients With Acute Biologic CrisisJames QuilingBelum ada peringkat
- Drug Study On Emergency DrugsDokumen14 halamanDrug Study On Emergency DrugsRene John FranciscoBelum ada peringkat
- Case Study-Pleural EffusionDokumen51 halamanCase Study-Pleural EffusionJames J. Salazar100% (4)
- Neonatologists' Pocket Drug Reference PDFDokumen185 halamanNeonatologists' Pocket Drug Reference PDFbaranclaudia100% (4)
- Fluids and Electrolytes - ExamDokumen6 halamanFluids and Electrolytes - ExamLouie Bello60% (5)
- Chapter 20: Drugs & Drug InteractionsDokumen18 halamanChapter 20: Drugs & Drug InteractionspoddataBelum ada peringkat
- Cardiac GlycosidesDokumen5 halamanCardiac Glycosidesapi-347182709100% (1)
- Drugs Used in Heart FailureDokumen33 halamanDrugs Used in Heart FailureLynx Kee Bayating100% (1)
- Unit-3 Full NotesDokumen15 halamanUnit-3 Full NotesABSOLUTE HABIBIBelum ada peringkat
- Chapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsDokumen5 halamanChapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsErika Joy Cabison TamayoBelum ada peringkat
- EKG StripsDokumen10 halamanEKG StripsSaidel ElizondoBelum ada peringkat
- 120DHA Questions With Correct Answers - 4 PDFDokumen12 halaman120DHA Questions With Correct Answers - 4 PDFAbdullah KdnlBelum ada peringkat
- Acls Prep Packet 2019aDokumen86 halamanAcls Prep Packet 2019aSanti ParambangBelum ada peringkat
- NLE Practice Exam With AnswersDokumen43 halamanNLE Practice Exam With AnswersSuzette Rae TateBelum ada peringkat
- HF and CAD Case ScenarioDokumen17 halamanHF and CAD Case ScenarioElla Neiza AngelesBelum ada peringkat
- BSN II Comprehensive Examination 2nd Sem 2017Dokumen12 halamanBSN II Comprehensive Examination 2nd Sem 2017Andrea Broccoli100% (1)
- C+F-Overview of Supraventriculer Tachycardia in Dogs and CatsDokumen11 halamanC+F-Overview of Supraventriculer Tachycardia in Dogs and Catstaner_soysurenBelum ada peringkat
- NCLEX Pharmacology Practice Exam W AnswersDokumen23 halamanNCLEX Pharmacology Practice Exam W Answersgregfocker57% (7)
- YeDokumen39 halamanYeRhea RaveloBelum ada peringkat
- Drugs Used in EmergencyDokumen7 halamanDrugs Used in EmergencyAzza DianBelum ada peringkat
- Module 8 PharmaDokumen34 halamanModule 8 PharmaGin MananganBelum ada peringkat
- 1,000 Questions To Help You Pass The Emergency Medicine BoardsDokumen338 halaman1,000 Questions To Help You Pass The Emergency Medicine Boardseric91% (11)
- Naplex 1Dokumen5 halamanNaplex 1Shan Shani100% (3)
- 5-Heart FailureDokumen12 halaman5-Heart FailureJericho De GuzmanBelum ada peringkat
- Review PharmacologyDokumen137 halamanReview PharmacologyGeronimo GonzalezBelum ada peringkat
- PNSG 214 Drug Research Assignment 2022 NewDokumen14 halamanPNSG 214 Drug Research Assignment 2022 Newapi-596613382Belum ada peringkat
- Moderately HighLY Protein Bound DrugsDokumen10 halamanModerately HighLY Protein Bound DrugsArah MomoBelum ada peringkat