Anda mungkin juga menyukai
- A-level Biology Revision: Cheeky Revision ShortcutsDari EverandA-level Biology Revision: Cheeky Revision ShortcutsPenilaian: 5 dari 5 bintang5/5 (5)
- Food Toxicology FSPT 2 YR. Food Toxicology FSPT 2 YR.: ND NDDokumen57 halamanFood Toxicology FSPT 2 YR. Food Toxicology FSPT 2 YR.: ND NDzekariyas kuneBelum ada peringkat
- Pharmacokinetics: "What The Body Does To The Drug"Dokumen41 halamanPharmacokinetics: "What The Body Does To The Drug"Virgo Eri SendiBelum ada peringkat
- Disposition of Toxic Compounds and Its Metabolic Reaction: 03/10/22 Toksikologi Lab. Biokimia Nutrisi 1Dokumen56 halamanDisposition of Toxic Compounds and Its Metabolic Reaction: 03/10/22 Toksikologi Lab. Biokimia Nutrisi 1Franco CibroBelum ada peringkat
- Disposition of ToxicantsDokumen102 halamanDisposition of ToxicantsApoorvi JainBelum ada peringkat
- Topic 5BDokumen70 halamanTopic 5BMohd RafiqBelum ada peringkat
- Toxicokinetics: Toxicokinetics Is Essentially The Study of "How ADokumen22 halamanToxicokinetics: Toxicokinetics Is Essentially The Study of "How ARajabMumbeeBelum ada peringkat
- Toxicology L3Dokumen24 halamanToxicology L3MA 09Belum ada peringkat
- 3 PharmacokineticsDokumen36 halaman3 PharmacokineticsTanvir FahimBelum ada peringkat
- Ico Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanDokumen34 halamanIco Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanMelkamu AyeBelum ada peringkat
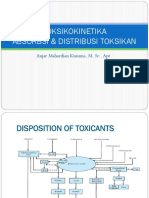
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDokumen51 halamanToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieBelum ada peringkat
- Absorption of DrugsDokumen41 halamanAbsorption of DrugsSibtain100% (2)
- Toxicokinetics: To It in The Body". Four Processes Are Involved in ToxicokineticsDokumen13 halamanToxicokinetics: To It in The Body". Four Processes Are Involved in ToxicokineticsSayed AlamBelum ada peringkat
- Pharmacokinetics: "What The Body Does To The Drug"Dokumen54 halamanPharmacokinetics: "What The Body Does To The Drug"Nur FadhilahBelum ada peringkat
- DR - Datten Bangun, MSC, SPFK Departemen Framakologi & Terapeutik Fakultas Kedokteran Universitas HKBP Nommensen MedanDokumen53 halamanDR - Datten Bangun, MSC, SPFK Departemen Framakologi & Terapeutik Fakultas Kedokteran Universitas HKBP Nommensen MedanSartika NapitupuluBelum ada peringkat
- BCH421. Biotransformation of XenobioticsDokumen8 halamanBCH421. Biotransformation of XenobioticsidriscognitoleadsBelum ada peringkat
- Unit 4 Factors Affecting Drug AbsorptionDokumen53 halamanUnit 4 Factors Affecting Drug Absorptiondiadiaida100% (1)
- Toxicokinetics DynamicsDokumen76 halamanToxicokinetics DynamicsSunil100% (1)
- Drug Absorption MechanismDokumen20 halamanDrug Absorption MechanismhabibieBelum ada peringkat
- Significance of ToxicokineticDokumen6 halamanSignificance of Toxicokineticlucy2 kasongiBelum ada peringkat
- Principles of Toxicology: The Study of PoisonsDokumen23 halamanPrinciples of Toxicology: The Study of PoisonsnitishkjhaBelum ada peringkat
- Biopharmaceutics and Clinical PharmacokineticsDokumen302 halamanBiopharmaceutics and Clinical PharmacokineticsBalisa MosisaBelum ada peringkat
- Toxicokinetics: "What The Body Does To The Toxic Material"Dokumen44 halamanToxicokinetics: "What The Body Does To The Toxic Material"Muhammad Shahid BilalBelum ada peringkat
- Continuous Antibiotic FermentationDokumen10 halamanContinuous Antibiotic FermentationJitendra MishraBelum ada peringkat
- GGDokumen24 halamanGGManan BhatiaBelum ada peringkat
- Kuliah FarmakologiDokumen74 halamanKuliah FarmakologiHanifBelum ada peringkat
- Pharmacokinetics (Absorption)Dokumen5 halamanPharmacokinetics (Absorption)okoroesther123Belum ada peringkat
- ADMEDokumen15 halamanADMEsachin kumarBelum ada peringkat
- Xenobiotics: Datta Meghe College of EngineeringDokumen33 halamanXenobiotics: Datta Meghe College of EngineeringsandeepBelum ada peringkat
- UNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Dokumen8 halamanUNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Hannah Jean Lapenid LemorenasBelum ada peringkat
- XenobioticsDokumen2 halamanXenobioticsKarthik SBelum ada peringkat
- Pharmacokinetics: Biological MembraneDokumen18 halamanPharmacokinetics: Biological MembraneRahul PalsBelum ada peringkat
- The Ladmer SystemDokumen12 halamanThe Ladmer Systemkriss WongBelum ada peringkat
- Day 7-8 ToxicityDokumen100 halamanDay 7-8 ToxicityAlfredoBelum ada peringkat
- 1introDokumen158 halaman1introDea MaharanisBelum ada peringkat
- Toxicokinetics and Toxicodynamics: DefinitionsDokumen7 halamanToxicokinetics and Toxicodynamics: DefinitionsquimicosorioBelum ada peringkat
- Drug Absorption: Dr. Chandane R. DDokumen54 halamanDrug Absorption: Dr. Chandane R. DBandameedi RamuBelum ada peringkat
- Distribution of DrugsDokumen36 halamanDistribution of DrugsKashar SaeedBelum ada peringkat
- SAAM-6636-001: Industrial Toxicology - Winter 2019 Class 4: Mechanisms of Toxicology Chapter 3 - Casarett and Doull'SDokumen16 halamanSAAM-6636-001: Industrial Toxicology - Winter 2019 Class 4: Mechanisms of Toxicology Chapter 3 - Casarett and Doull'Skriz0812Belum ada peringkat
- Bio TransformationDokumen16 halamanBio Transformationrawatpooran05Belum ada peringkat
- Xenobiotics in Biological SystemsDokumen11 halamanXenobiotics in Biological SystemsG S MalhotraBelum ada peringkat
- 1.1.1 Pharmacokinetics 2022 - 2023Dokumen65 halaman1.1.1 Pharmacokinetics 2022 - 2023brightgyan082Belum ada peringkat
- 1.pharmacology OpeningDokumen6 halaman1.pharmacology OpeningHOPEBelum ada peringkat
- Pharmaco KineticsDokumen69 halamanPharmaco KineticsSristeeBelum ada peringkat
- Pharmacokinetics - 1Dokumen41 halamanPharmacokinetics - 1SristeeBelum ada peringkat
- Pharmaco KineticsDokumen42 halamanPharmaco KineticsNaghman ZuberiBelum ada peringkat
- Neeraj Assignment PDFDokumen68 halamanNeeraj Assignment PDFNeeraj GautamBelum ada peringkat
- Drug Absorption 01Dokumen15 halamanDrug Absorption 01Jannaatul Ferdous MimBelum ada peringkat
- Drug Metabolism ADME PrincipalDokumen38 halamanDrug Metabolism ADME PrincipalA. Kumar Soni100% (1)
- Resumen FarmacoDokumen9 halamanResumen FarmacoMagali DelvalleBelum ada peringkat
- Pharmaco KineticsDokumen10 halamanPharmaco KineticsVithyaah ParameswaranBelum ada peringkat
- TOXICOLOGY Solvents and Vapors 20240418 112830 0000Dokumen30 halamanTOXICOLOGY Solvents and Vapors 20240418 112830 0000Trisha Mae Fernandez AustriaBelum ada peringkat
- 3.unit - Pharmacokinetics 2Dokumen40 halaman3.unit - Pharmacokinetics 22020253350Belum ada peringkat
- Chapter 2 - Absorption - RevisedDokumen130 halamanChapter 2 - Absorption - RevisedMinal NadeemBelum ada peringkat
- Microbial GrowthDokumen54 halamanMicrobial GrowthLeen ShalabiBelum ada peringkat
- Xenobiotic FKBiotransformationDokumen100 halamanXenobiotic FKBiotransformationMuhammad SyaifullahBelum ada peringkat
- Analysis of Xenobiotics: A Review: ArticleDokumen8 halamanAnalysis of Xenobiotics: A Review: ArticleYoravika dwiwibanggaBelum ada peringkat
- Biopharmaceutics and Clinical Pharmacokinetics - 20210831 - 212949Dokumen22 halamanBiopharmaceutics and Clinical Pharmacokinetics - 20210831 - 212949Md. Abu Bakar Siddique TayefBelum ada peringkat
- HomeostasisDokumen13 halamanHomeostasisSanchezBelum ada peringkat
- Nouns and QuantifiersDokumen6 halamanNouns and QuantifiersAsyraf RefdinBelum ada peringkat
- Table 1: Water Quality Parameter and Standard: American Journal of Agricultural ScienceDokumen1 halamanTable 1: Water Quality Parameter and Standard: American Journal of Agricultural ScienceAsyraf RefdinBelum ada peringkat
- Activities: Semester 1 Feb MarchDokumen16 halamanActivities: Semester 1 Feb MarchAsyraf RefdinBelum ada peringkat
- Pips Technical Service Price ListDokumen5 halamanPips Technical Service Price ListAsyraf RefdinBelum ada peringkat
- ASSIST - Indicator For Testing For Water Hardness - 2019-02-22Dokumen6 halamanASSIST - Indicator For Testing For Water Hardness - 2019-02-22Asyraf RefdinBelum ada peringkat
- Jadual Pertandingan Liga Dan Kalah Mati FutsalDokumen2 halamanJadual Pertandingan Liga Dan Kalah Mati FutsalAsyraf RefdinBelum ada peringkat
- Geographical Information System Lab PracticalDokumen2 halamanGeographical Information System Lab PracticalAsyraf RefdinBelum ada peringkat
- Tutorial 4 DerivativeDokumen2 halamanTutorial 4 DerivativeAsyraf RefdinBelum ada peringkat
- Summary BookDokumen1 halamanSummary BookAsyraf RefdinBelum ada peringkat
- Beauty and The Beast by Celine DionDokumen1 halamanBeauty and The Beast by Celine DionAsyraf RefdinBelum ada peringkat
- Discussion Heavy Metal Air QualityDokumen7 halamanDiscussion Heavy Metal Air QualityAsyraf RefdinBelum ada peringkat
- Qmt245 CourseDokumen3 halamanQmt245 CourseAsyraf RefdinBelum ada peringkat
- Conclusion Malay LanguageDokumen1 halamanConclusion Malay LanguageAsyraf RefdinBelum ada peringkat
- Tutorial 7Dokumen1 halamanTutorial 7Asyraf RefdinBelum ada peringkat
- Tutorial 1Dokumen3 halamanTutorial 1Asyraf RefdinBelum ada peringkat
- SZA/PHY 210/ 2013: 0.45 Cos 6.40tDokumen2 halamanSZA/PHY 210/ 2013: 0.45 Cos 6.40tAsyraf RefdinBelum ada peringkat
- Tutorial 1Dokumen3 halamanTutorial 1Asyraf RefdinBelum ada peringkat
- Show That For Function F Defined By: Calculus Worksheet: Continuity of FunctionsDokumen1 halamanShow That For Function F Defined By: Calculus Worksheet: Continuity of FunctionsAsyraf RefdinBelum ada peringkat
- Tips and Prediction SPM 2012Dokumen5 halamanTips and Prediction SPM 2012Asyraf RefdinBelum ada peringkat
- 2017 - Behavioral Emergencies - Geriatric Psychiatric PatientDokumen14 halaman2017 - Behavioral Emergencies - Geriatric Psychiatric PatientAna María Arenas DávilaBelum ada peringkat
- Soil MechDokumen21 halamanSoil MechAhsan AbbasBelum ada peringkat
- Architecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Dokumen6 halamanArchitecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Asmaa AyadBelum ada peringkat
- My Personal Brand and Career GoalsDokumen3 halamanMy Personal Brand and Career GoalsPhúc ĐàoBelum ada peringkat
- Lesson 11Dokumen3 halamanLesson 11Jhoanna Rose AlingalanBelum ada peringkat
- Thesis TopicsDokumen9 halamanThesis TopicsInayath AliBelum ada peringkat
- SSP 861603 - EN - Tire Pressure Monitoring SystemsDokumen42 halamanSSP 861603 - EN - Tire Pressure Monitoring Systemsa.diedrichsBelum ada peringkat
- Q&A FractureDokumen13 halamanQ&A FractureRed JimenoBelum ada peringkat
- Bajaj Holdings & Investment Ltd. - Research Center: Balance SheetDokumen6 halamanBajaj Holdings & Investment Ltd. - Research Center: Balance Sheetsarathkumarreddy855081Belum ada peringkat
- The Appropriate Biochemical Oxygen Demand Concentration For Designing Domestic Wastewater Treatment PlantDokumen8 halamanThe Appropriate Biochemical Oxygen Demand Concentration For Designing Domestic Wastewater Treatment PlantabdulBelum ada peringkat
- LEASE CONTRACT Taytay Residentialhouse Kei Inagaki Nena TrusaDokumen6 halamanLEASE CONTRACT Taytay Residentialhouse Kei Inagaki Nena TrusaJaime GonzalesBelum ada peringkat
- Melo V PeopleDokumen1 halamanMelo V PeoplejjangBelum ada peringkat
- Comparative Analysis of Motivation TheoriesDokumen14 halamanComparative Analysis of Motivation TheoriesNomvelo MajolaBelum ada peringkat
- 2016-FL3030说明书50m臂长最后版-2016 11 3 PDFDokumen96 halaman2016-FL3030说明书50m臂长最后版-2016 11 3 PDFMohammed SumerBelum ada peringkat
- This Study Resource WasDokumen2 halamanThis Study Resource Waskaye nicolasBelum ada peringkat
- Urban Square Design: Landscape Design Studio III LAR 803Dokumen44 halamanUrban Square Design: Landscape Design Studio III LAR 803Peter DokpesiBelum ada peringkat
- Tutorial 2 - Financial EnvironmentDokumen5 halamanTutorial 2 - Financial EnvironmentShi ManBelum ada peringkat
- 10 Rules of Statcon by Atty Marcus NeelyDokumen4 halaman10 Rules of Statcon by Atty Marcus NeelyMorin OcoBelum ada peringkat
- Detailed Lesson Plan in HousekeepingDokumen6 halamanDetailed Lesson Plan in HousekeepingreyBelum ada peringkat
- Modfied Indian Systems of MedicineDokumen8 halamanModfied Indian Systems of MedicineNishamolKSBelum ada peringkat
- Program 2019 MTAPTL Annual Convention PDFDokumen3 halamanProgram 2019 MTAPTL Annual Convention PDFrichardlfigueroaBelum ada peringkat
- Part D - Disclosure and TransparencyDokumen21 halamanPart D - Disclosure and TransparencyMuhammadYudithEddwinaBelum ada peringkat
- Coca Cola FSDokumen3 halamanCoca Cola FSManan MunshiBelum ada peringkat
- Commentary On The Book of NahumDokumen9 halamanCommentary On The Book of NahumRev Dr Jeffry Camm JP, MIEPR, MISOPBelum ada peringkat
- dnd3 Character Sheet STD 105cDokumen2 halamandnd3 Character Sheet STD 105cGerry MaloneyBelum ada peringkat
- Midterm Test 1Dokumen3 halamanMidterm Test 1Hùng Trường NguyễnBelum ada peringkat
- Expanding The Product Range of Leena by Bata (Report)Dokumen104 halamanExpanding The Product Range of Leena by Bata (Report)Rabya TauheedBelum ada peringkat
- (EN) Google Developer Policy - September 1, 2021Dokumen56 halaman(EN) Google Developer Policy - September 1, 2021JimmyBelum ada peringkat
- INSTRUCTIONS FOR USOL PRIVATE REAPPEAR DE January 2022Dokumen4 halamanINSTRUCTIONS FOR USOL PRIVATE REAPPEAR DE January 2022RaghavBelum ada peringkat
- 1.2 Introduction To PHP - PHP KeywordsDokumen12 halaman1.2 Introduction To PHP - PHP KeywordsOvie Nur FaizahBelum ada peringkat