Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Anatomy and Physiology of Respiratory SystemDokumen9 halamanAnatomy and Physiology of Respiratory SystemLiza Marie Cayetano AdarneBelum ada peringkat
- List of Geometric CardsDokumen102 halamanList of Geometric CardsamazingdivinegraceBelum ada peringkat
- Lab Report Bio Experiment 3 - Reproductive, Endocrine & Respiratory System (Group 4)Dokumen15 halamanLab Report Bio Experiment 3 - Reproductive, Endocrine & Respiratory System (Group 4)FARHAH BATRISYIA ABDUL RAHIMBelum ada peringkat
- Marmas Shamana Oils 2 10 11Dokumen7 halamanMarmas Shamana Oils 2 10 11anatugario100% (1)
- Nursing Care Plan For Pneumonia NCPDokumen2 halamanNursing Care Plan For Pneumonia NCPRoger Jr PumarenBelum ada peringkat
- 118 Skills Lab-Week 1-Responses To Altered Ventilatory FunctionsDokumen8 halaman118 Skills Lab-Week 1-Responses To Altered Ventilatory FunctionsKeisha BartolataBelum ada peringkat
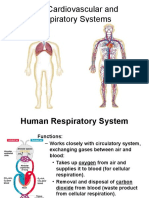
- Cardiovascular and Respiratory SystemDokumen51 halamanCardiovascular and Respiratory SystemKarel Mae SanoriaBelum ada peringkat
- Case StudyDokumen43 halamanCase StudyElena Cariño De Guzman100% (1)
- HSNS264 Assessment 1Dokumen6 halamanHSNS264 Assessment 1Sophie AndersonBelum ada peringkat
- Pulmonary Tuberculosis Case PresentationDokumen71 halamanPulmonary Tuberculosis Case PresentationSimeonDomingoTorresSy100% (4)
- Paper13 PDFDokumen6 halamanPaper13 PDFSekar MentariBelum ada peringkat
- The Triple Elimination of Mother-to-Child Transmission of HIV, Hepatitis B and Syphilis in Asia and The Pacific, 2018-2030Dokumen44 halamanThe Triple Elimination of Mother-to-Child Transmission of HIV, Hepatitis B and Syphilis in Asia and The Pacific, 2018-2030Sekar MentariBelum ada peringkat
- Jurnal Kebijakan Kesehatan IndonesiaDokumen8 halamanJurnal Kebijakan Kesehatan IndonesiaSekar MentariBelum ada peringkat
- Radiographic Diagnosis of Hyaline Membrane Disease'Dokumen5 halamanRadiographic Diagnosis of Hyaline Membrane Disease'Sekar MentariBelum ada peringkat
- Dinda Anggita M - Microteaching - Class XI - Respiratory SystemDokumen20 halamanDinda Anggita M - Microteaching - Class XI - Respiratory SystemdindaBelum ada peringkat
- Respiratory Distress SyndromeDokumen69 halamanRespiratory Distress SyndromeAbraham ChiuBelum ada peringkat
- Respiratory SystemDokumen89 halamanRespiratory SystemMuhammad HanifBelum ada peringkat
- Chest X-Ray (CXR) Interpretation 2Dokumen30 halamanChest X-Ray (CXR) Interpretation 2NaveedBelum ada peringkat
- ANAT3007 Lower Respiratory System & Diaphragm Lecture Notes MBG2023Dokumen48 halamanANAT3007 Lower Respiratory System & Diaphragm Lecture Notes MBG2023RachaelBelum ada peringkat
- Class Lesson - Lesson 2. Respiratory SystemDokumen18 halamanClass Lesson - Lesson 2. Respiratory Systemshellers24Belum ada peringkat
- Massive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFDokumen21 halamanMassive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFdoc_next_doorBelum ada peringkat
- Anatomy of Lung, Pleura, Surface MarkingDokumen22 halamanAnatomy of Lung, Pleura, Surface MarkingSandhya SureshBelum ada peringkat
- Gas Exchange in HumansDokumen38 halamanGas Exchange in HumansGift Blessed NgoveBelum ada peringkat
- Pulmonary Pathology: Maria Sarah L. Lenon, MD, DPSPDokumen32 halamanPulmonary Pathology: Maria Sarah L. Lenon, MD, DPSPKATREEYA ELEONOR LIMSIBelum ada peringkat
- Boyden 1953Dokumen10 halamanBoyden 1953Giancarlo Maruri MunarettoBelum ada peringkat
- A Case Study ON Pneumonia: Panpacific University North PhilippinesDokumen13 halamanA Case Study ON Pneumonia: Panpacific University North PhilippinesAbdalrahman AhmedBelum ada peringkat
- Interstitial Vs AlveolarDokumen17 halamanInterstitial Vs AlveolarEdwin DarmawanBelum ada peringkat
- Avian Medicine:: Principles and ApplicationDokumen27 halamanAvian Medicine:: Principles and ApplicationMito M GaviriaBelum ada peringkat
- Gas Exchange in Humans 1 MSDokumen6 halamanGas Exchange in Humans 1 MSKatlego MedupeBelum ada peringkat
- Coughing in DogsDokumen7 halamanCoughing in DogsCristina RizkallalBelum ada peringkat
- Respiratory SystemDokumen25 halamanRespiratory Systemlobna HijliBelum ada peringkat
- Тopic 4.2. Auscultation of the lungs. Additional sounds.Dokumen7 halamanТopic 4.2. Auscultation of the lungs. Additional sounds.Donia HnainiaBelum ada peringkat
- Human Physiology 01 - Theory Notes - PDF Only - NSEJS 2023Dokumen94 halamanHuman Physiology 01 - Theory Notes - PDF Only - NSEJS 2023Chinmay GoelBelum ada peringkat
- The Respiratory SystemDokumen3 halamanThe Respiratory Systempaulo_camuaBelum ada peringkat