Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Noiseless Pavements: by Jestin John B110286CEDokumen26 halamanNoiseless Pavements: by Jestin John B110286CEAnilkmar P M80% (5)
- Ethical Issues in CP: By: Yemataw Wondie, PHDDokumen32 halamanEthical Issues in CP: By: Yemataw Wondie, PHDdawit girmaBelum ada peringkat
- Relationship of Habitual Dietary Intake and Mood of Medical Students of Uermmmci: A Cross-Sectional StudyDokumen1 halamanRelationship of Habitual Dietary Intake and Mood of Medical Students of Uermmmci: A Cross-Sectional Studyhfjs alOqfvaBelum ada peringkat
- Alternative MedicineDokumen306 halamanAlternative MedicineDamir Brankovic100% (3)
- Ig1 Igc1 0005 Eng Obe Answer Sheet v1Dokumen5 halamanIg1 Igc1 0005 Eng Obe Answer Sheet v1FARHAN50% (2)
- Grand FCS A Chap 6Dokumen38 halamanGrand FCS A Chap 6Katherine 'Chingboo' Leonico LaudBelum ada peringkat
- Fasting Blood SugarDokumen5 halamanFasting Blood SugarKhamron BridgewaterBelum ada peringkat
- The Nutrition Care Process Related To HypertensionDokumen22 halamanThe Nutrition Care Process Related To HypertensionNita SeptianaBelum ada peringkat
- Inclusion WorksDokumen94 halamanInclusion WorksAlvaro MejiaBelum ada peringkat
- Studentsworksheets PbirevisedDokumen8 halamanStudentsworksheets Pbirevisedapi-246444495Belum ada peringkat
- Dental Health 2017Dokumen1 halamanDental Health 2017coloradoresourcesBelum ada peringkat
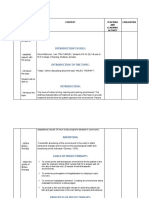
- Introduction To Self:: Time Specific Objective Content Teaching AND Learning Activity EvaluationDokumen20 halamanIntroduction To Self:: Time Specific Objective Content Teaching AND Learning Activity EvaluationKiran Kour100% (2)
- Initial Nurse Patient InteractionDokumen1 halamanInitial Nurse Patient InteractionBryan Jay Carlo PañaBelum ada peringkat
- MGDS III Draft - August - Ed.final Final 16.08.17 (Sam)Dokumen236 halamanMGDS III Draft - August - Ed.final Final 16.08.17 (Sam)AngellaBelum ada peringkat
- C Section: Students: Modiga Daria Moneanu Anda Nica Maria-CristinaDokumen11 halamanC Section: Students: Modiga Daria Moneanu Anda Nica Maria-CristinaDaria Modiga100% (1)
- Positions For Labour and BirthDokumen9 halamanPositions For Labour and BirthVandi ChiemropsBelum ada peringkat
- Drug StudyDokumen13 halamanDrug StudygemzkeeBelum ada peringkat
- Care of The Newborn PDFDokumen5 halamanCare of The Newborn PDFzhai bambalan100% (2)
- Vibitha Joseph Naramvelil: Compassionate - Rehabilitation and Home Care Experience - MultilingualDokumen3 halamanVibitha Joseph Naramvelil: Compassionate - Rehabilitation and Home Care Experience - MultilingualSanish ScariaBelum ada peringkat
- Disseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractDokumen3 halamanDisseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractAmelia Fitria DewiBelum ada peringkat
- Microsoft PowerPoint - KNUST-LECT-STUDENT MALARIA (Compatibility Mode)Dokumen9 halamanMicrosoft PowerPoint - KNUST-LECT-STUDENT MALARIA (Compatibility Mode)AnastasiafynnBelum ada peringkat
- Christian Christopher D. Lopez: Dapitan City Municipality of Sapang DalagaDokumen3 halamanChristian Christopher D. Lopez: Dapitan City Municipality of Sapang DalagaChristian Christopher LopezBelum ada peringkat
- Hemodialysis Clinic Assessment ToolDokumen5 halamanHemodialysis Clinic Assessment ToolAn-Nisa Khoirun UmmiBelum ada peringkat
- Negative Effects of Technology On Child Development - Carolina PerezDokumen6 halamanNegative Effects of Technology On Child Development - Carolina PerezCarolina PerezBelum ada peringkat
- Family As A Unit of Care-1Dokumen17 halamanFamily As A Unit of Care-1Kim RamosBelum ada peringkat
- Swimming Is The Self-Propulsion of A Person Through WaterDokumen3 halamanSwimming Is The Self-Propulsion of A Person Through WaterKryzler KayeBelum ada peringkat
- Food Poisoning: DR Muhammad Isya Firmansyah MDDokumen26 halamanFood Poisoning: DR Muhammad Isya Firmansyah MDilo nurseBelum ada peringkat
- III. Nursing Care Plan Nursing Priority No. 1: Ineffective Airway Clearance Related To Excessive Accumulation of Secretions Secondary To PneumoniaDokumen6 halamanIII. Nursing Care Plan Nursing Priority No. 1: Ineffective Airway Clearance Related To Excessive Accumulation of Secretions Secondary To PneumoniaRae Marie Aquino100% (1)
- CELYN H. NATURAL MAPEH LESSON PLAN (MR - Gepitulan)Dokumen6 halamanCELYN H. NATURAL MAPEH LESSON PLAN (MR - Gepitulan)Celyn NaturalBelum ada peringkat
- Puerperal SepsisDokumen45 halamanPuerperal SepsisKalo kajiBelum ada peringkat