Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Ecg Workout PDFDokumen419 halamanEcg Workout PDFawinsy100% (4)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- 01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFDokumen26 halaman01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFawinsyBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Angina Pectoris Treatment & Management - Medical Care, Surgical Care, PreventionDokumen20 halamanAngina Pectoris Treatment & Management - Medical Care, Surgical Care, Preventionblack_eagel100% (1)
- The Expanded Family Life Cycle - Individual, Family, and Social Perspectives PDFDokumen501 halamanThe Expanded Family Life Cycle - Individual, Family, and Social Perspectives PDFawinsy93% (15)
- Research For Nurses - Methods and InterpretationDokumen767 halamanResearch For Nurses - Methods and Interpretationawinsy100% (1)
- Emergency MedicineDokumen150 halamanEmergency MedicineDev MartelBelum ada peringkat
- A Case Presentation of An Adult With Gestational Diabetes MellitusDokumen56 halamanA Case Presentation of An Adult With Gestational Diabetes MellitusAnn Mariz Dominguez100% (5)
- Plum and Posner's Diagnosis of Stupor and ComaDokumen416 halamanPlum and Posner's Diagnosis of Stupor and Comakikotido8100% (1)
- TOEFL - GrammarDokumen221 halamanTOEFL - Grammarcharlesbl100% (4)
- Leadership Styles in NursingDokumen10 halamanLeadership Styles in NursingawinsyBelum ada peringkat
- Chapter 48 Neonatal and Pediatric Respiratory CareDokumen6 halamanChapter 48 Neonatal and Pediatric Respiratory CareMM Ayehsa Allian SchückBelum ada peringkat
- 01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFDokumen26 halaman01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFawinsyBelum ada peringkat
- Fosphenytoin - A Feasible Alternative To Phenytoin For Seizure TherapyDokumen2 halamanFosphenytoin - A Feasible Alternative To Phenytoin For Seizure TherapyawinsyBelum ada peringkat
- The Top 10 Pitfalls To Avoid When Caring For The Older Adult - Part IDokumen3 halamanThe Top 10 Pitfalls To Avoid When Caring For The Older Adult - Part IawinsyBelum ada peringkat
- Recognizing Pain As A Component of The Primary Assessment - Adding D For Discomfort To The ABCs PDFDokumen6 halamanRecognizing Pain As A Component of The Primary Assessment - Adding D For Discomfort To The ABCs PDFawinsyBelum ada peringkat
- An Overview of Magnesium Use in The Emergency Department PDFDokumen8 halamanAn Overview of Magnesium Use in The Emergency Department PDFawinsyBelum ada peringkat
- Fear As A Property and An Entitlement - Humphrey 2013 PDFDokumen20 halamanFear As A Property and An Entitlement - Humphrey 2013 PDFawinsyBelum ada peringkat
- Fear As A Disposition and An Emotional State: A Genetic and Environmental Approach To Out-Group Political PreferencesDokumen15 halamanFear As A Disposition and An Emotional State: A Genetic and Environmental Approach To Out-Group Political PreferencesawinsyBelum ada peringkat
- The Amygdala PDFDokumen7 halamanThe Amygdala PDFawinsyBelum ada peringkat
- Nice Guideline Blood Transfusion PDFDokumen28 halamanNice Guideline Blood Transfusion PDFawinsyBelum ada peringkat
- The Amygdala PDFDokumen7 halamanThe Amygdala PDFawinsyBelum ada peringkat
- Conocimiento en EnfermeriaDokumen4 halamanConocimiento en EnfermeriaawinsyBelum ada peringkat
- Nursing Interventions For Identifying and Managing Acute Dysphagia Are Effective For Improving Patient OutcomesDokumen9 halamanNursing Interventions For Identifying and Managing Acute Dysphagia Are Effective For Improving Patient OutcomesawinsyBelum ada peringkat
- Adam Worcester-Building Grammar Skills For TOEFL IBTDokumen221 halamanAdam Worcester-Building Grammar Skills For TOEFL IBTawinsyBelum ada peringkat
- Ecomapping - An Innovative Research Tool For NursesDokumen8 halamanEcomapping - An Innovative Research Tool For NursesawinsyBelum ada peringkat
- Nursing Epistemology - Traditions, Insights, QuestionsDokumen5 halamanNursing Epistemology - Traditions, Insights, Questionsawinsy100% (1)
- Epilepsia Frontal DorsolateralDokumen6 halamanEpilepsia Frontal DorsolateralawinsyBelum ada peringkat
- Anxiety, Stress and Coping Behaviours in Primary Care Migraine Patients - Results of The SMILE StudyDokumen11 halamanAnxiety, Stress and Coping Behaviours in Primary Care Migraine Patients - Results of The SMILE StudyawinsyBelum ada peringkat
- Caring For A Family Member With Intellectual Disability and Epilepsy - Practical, Social and Emotional PerspectivesDokumen8 halamanCaring For A Family Member With Intellectual Disability and Epilepsy - Practical, Social and Emotional PerspectivesawinsyBelum ada peringkat
- Coping With Epilepsy - The Effect of Coping Styles On Self-Perceived Seizure Severity and Psychological ComplaintsDokumen4 halamanCoping With Epilepsy - The Effect of Coping Styles On Self-Perceived Seizure Severity and Psychological ComplaintsawinsyBelum ada peringkat
- Vagus Nerve Stimulation Therapy For Pharmacoresistant EpilepsyDokumen5 halamanVagus Nerve Stimulation Therapy For Pharmacoresistant EpilepsyawinsyBelum ada peringkat
- Approach To The Comatose Patient. CCM Jan 06Dokumen11 halamanApproach To The Comatose Patient. CCM Jan 06awinsyBelum ada peringkat
- WOQOL Measuring QV MentalDokumen15 halamanWOQOL Measuring QV MentalpenfoBelum ada peringkat
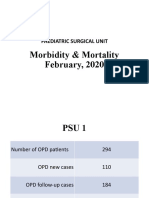
- Morbidity & Mortality (February, 2020)Dokumen14 halamanMorbidity & Mortality (February, 2020)Wai GyiBelum ada peringkat
- Dwnload Full Little and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank PDFDokumen36 halamanDwnload Full Little and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank PDFdanagarzad90y100% (10)
- Dokumen Tanpa JudulDokumen11 halamanDokumen Tanpa JudulRabiatul adhwiyah DalimuntheBelum ada peringkat
- Biology: Pearson EdexcelDokumen32 halamanBiology: Pearson Edexcelbody fayez100% (1)
- SGD Im Group 1c Final PresentationDokumen54 halamanSGD Im Group 1c Final Presentationnachiketpanchal8Belum ada peringkat
- Lithium: Mimicry, Mania, and Muscle Relaxants: Simon Flood MRCP FRCA Andrew Bodenham FRCADokumen4 halamanLithium: Mimicry, Mania, and Muscle Relaxants: Simon Flood MRCP FRCA Andrew Bodenham FRCARizwan AhmedBelum ada peringkat
- Frog ALL SYSTEMS-1Dokumen85 halamanFrog ALL SYSTEMS-1Ranjeet PandeyBelum ada peringkat
- Neoreviews 201533Dokumen11 halamanNeoreviews 201533Dmitri KaramazovBelum ada peringkat
- Mina NotesDokumen649 halamanMina Notestoobakhann23Belum ada peringkat
- Basic EP IntervalsDokumen13 halamanBasic EP IntervalsdrharoonmohdBelum ada peringkat
- Clinical Manifestations and Diagnosis of Vitamin B12 and Folate Deficiency - UpToDateDokumen63 halamanClinical Manifestations and Diagnosis of Vitamin B12 and Folate Deficiency - UpToDateHuỳnh Thị Khả DuyBelum ada peringkat
- Introduction To Global Health 2nd Edition Jacobsen Test BankDokumen5 halamanIntroduction To Global Health 2nd Edition Jacobsen Test Banksinhhanhi7rp100% (28)
- The Fontan Circulation Contin EducDokumen5 halamanThe Fontan Circulation Contin EducAishu BBelum ada peringkat
- Pneumonia, BronchiolitisDokumen65 halamanPneumonia, BronchiolitisYemata HailuBelum ada peringkat
- NS2881 Renal Revision Worksheet 2022Dokumen10 halamanNS2881 Renal Revision Worksheet 2022Louise GeislerBelum ada peringkat
- JCM 12 01482 v2 PDFDokumen11 halamanJCM 12 01482 v2 PDFPutra FhonnaBelum ada peringkat
- 11 Anti-Coagulants & FibrinolyticsDokumen52 halaman11 Anti-Coagulants & FibrinolyticsUmmuShefaBelum ada peringkat
- Final Coaching CardioDokumen70 halamanFinal Coaching CardiomarykristiroseBelum ada peringkat
- ZOOL30040 Practical HandoutDokumen10 halamanZOOL30040 Practical Handoutannabelledarcy247Belum ada peringkat
- Jurnal Cardiac RhabdomyomaDokumen12 halamanJurnal Cardiac Rhabdomyomamagda goeyBelum ada peringkat
- DiastologiaDokumen10 halamanDiastologiaReinaldo Pacheco VásquezBelum ada peringkat
- Amlodipine ReadingDokumen12 halamanAmlodipine Readingines pachecoBelum ada peringkat
- 7 Urinary Disorders - 2012 - Small Animal Clinical Diagnosis by Laboratory Methods Fifth EditionDokumen30 halaman7 Urinary Disorders - 2012 - Small Animal Clinical Diagnosis by Laboratory Methods Fifth EditionNarvarte Hospital Veterinario de EspecialidadesBelum ada peringkat
- Supraventricular TachycardiaDokumen7 halamanSupraventricular Tachycardiaagarrido2Belum ada peringkat
- MRCP Part 1 SyllabusDokumen18 halamanMRCP Part 1 SyllabusAggamemnon populosBelum ada peringkat
- Surgery 5th SEM MCQs AnsDokumen75 halamanSurgery 5th SEM MCQs Anskthangjam21Belum ada peringkat