Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Dr. AVISSENA - The Basics of Immunotherapy in CancerDokumen24 halamanDr. AVISSENA - The Basics of Immunotherapy in CancerAlbertus Aditya BudiyantoBelum ada peringkat
- C P A G F A Q (Faq) F P P MDokumen2 halamanC P A G F A Q (Faq) F P P MDewanggaWahyuPrajaBelum ada peringkat
- Booklet KasarDokumen28 halamanBooklet KasarAlbertus Aditya BudiyantoBelum ada peringkat
- Multiple Myeloma With PathophysiologyDokumen32 halamanMultiple Myeloma With Pathophysiologymabec pagaduan90% (10)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Manuscript For ReviewDokumen10 halamanManuscript For ReviewAliMohamadBelum ada peringkat
- 2016-04-15 Banjarmasin DisolfDokumen41 halaman2016-04-15 Banjarmasin DisolffaisalsyahrilBelum ada peringkat
- MLS 12aa: Hematology 2 (Laboratory) : Module 2: Bleeding Time and Clottinfg TimeDokumen9 halamanMLS 12aa: Hematology 2 (Laboratory) : Module 2: Bleeding Time and Clottinfg TimeRuphele Anne Quitag100% (1)
- Hema2 Lec 2 TransDokumen159 halamanHema2 Lec 2 TransJPBelum ada peringkat
- Risk For BleedingDokumen2 halamanRisk For Bleedingmikebry72% (25)
- Biochem Ratio 7 FinalDokumen31 halamanBiochem Ratio 7 FinalJimell ObradorBelum ada peringkat
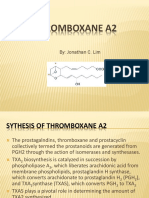
- Thromboxane A2Dokumen16 halamanThromboxane A2Concepcion R. Aquino0% (1)
- Richards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023Dokumen13 halamanRichards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023jorge fabregatBelum ada peringkat
- Circulatory SystemDokumen21 halamanCirculatory SystemYusuf AzeezBelum ada peringkat
- Severe Thrombocytopenia Secondary To Alcohol Use Article JournalDokumen3 halamanSevere Thrombocytopenia Secondary To Alcohol Use Article JournalAulia ZrBelum ada peringkat
- 2019 Modified Blood ComponentsDokumen30 halaman2019 Modified Blood Componentsسعد الطائعBelum ada peringkat
- Hemostasis and Coagulation: Miklós MolnárDokumen67 halamanHemostasis and Coagulation: Miklós MolnárHamzaBelum ada peringkat
- PASTEST Total Revision Ear, Nose and ThroatDokumen391 halamanPASTEST Total Revision Ear, Nose and Throatathiya nadifaBelum ada peringkat
- HematopoiesisDokumen8 halamanHematopoiesisCassandra Grace Labial PaynterBelum ada peringkat
- Tabung Vakum PDFDokumen14 halamanTabung Vakum PDFGilang NugrahaBelum ada peringkat
- Surgery Examination - 3-4 (Question Cases) (Eng)Dokumen45 halamanSurgery Examination - 3-4 (Question Cases) (Eng)Aiman TymerBelum ada peringkat
- Wa0038.Dokumen9 halamanWa0038.Sambhu Nath DeyBelum ada peringkat
- 2021 L Two PhysiologyofbloodDokumen22 halaman2021 L Two PhysiologyofbloodOKUDRA GEOFRYBelum ada peringkat
- Review of Current Transfusion Therapy and Blood Banking PracticesDokumen52 halamanReview of Current Transfusion Therapy and Blood Banking PracticesAmaranto SantosoBelum ada peringkat
- The Wound Healing ProcessDokumen15 halamanThe Wound Healing Processtabris76Belum ada peringkat
- Science f3 UB1Dokumen7 halamanScience f3 UB1LEENA HingBelum ada peringkat
- Dengue Hemorrhagic FeverDokumen68 halamanDengue Hemorrhagic FeverClaire Gentallan50% (2)
- Stanpad CatalogDokumen2 halamanStanpad CatalogSUBEKTIBelum ada peringkat
- On GK-HP2Dokumen3 halamanOn GK-HP2Kieu AnhBelum ada peringkat
- Component & Effective Use of BloodDokumen56 halamanComponent & Effective Use of BloodNorlelawati TalibBelum ada peringkat
- Why Leech TherpyDokumen11 halamanWhy Leech TherpyAbhishek Tayal100% (1)
- Lecture 4-HemostasisDokumen34 halamanLecture 4-HemostasissamayaBelum ada peringkat
- Hemostaza LPDokumen12 halamanHemostaza LPmoto24100% (1)
- PLT MeasurementsDokumen6 halamanPLT MeasurementsAudreySlitBelum ada peringkat
- Overview of The Coagulation SystemDokumen9 halamanOverview of The Coagulation SystemaksinuBelum ada peringkat