Anda mungkin juga menyukai
- UntitledDokumen49 halamanUntitledkedas70Belum ada peringkat
- UntitledDokumen56 halamanUntitledkedas70Belum ada peringkat
- Fast Facts: Enfermedad inflamatoria intestinal Para Pacientes y las Personas que los Apoyan: Colitis ulcerativa y enfermedad de Crohn Información + Tomar el control = El mejor resultadoDari EverandFast Facts: Enfermedad inflamatoria intestinal Para Pacientes y las Personas que los Apoyan: Colitis ulcerativa y enfermedad de Crohn Información + Tomar el control = El mejor resultadoBelum ada peringkat
- Diseases of Small and Large IntestineDokumen20 halamanDiseases of Small and Large IntestineOluwagbemisoke Estherr OlatunjiBelum ada peringkat
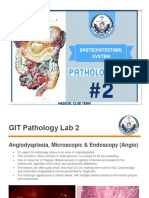
- Practical No 29 - Gastrointestinal TractDokumen7 halamanPractical No 29 - Gastrointestinal Tractkartik.patil151106Belum ada peringkat
- Appendix Part 1Dokumen8 halamanAppendix Part 1Abdullah EssaBelum ada peringkat
- Pathology of Small & Large Intestine: Developmental LesionsDokumen5 halamanPathology of Small & Large Intestine: Developmental LesionsaiadalkhalidiBelum ada peringkat
- Inflammatory Bowel Disease: Ruchita BhavsarDokumen34 halamanInflammatory Bowel Disease: Ruchita BhavsarShinta MayasariBelum ada peringkat
- Peptic and Other Benign UlcersDokumen31 halamanPeptic and Other Benign Ulcersmomi311Belum ada peringkat
- UntitledDokumen49 halamanUntitledkedas70Belum ada peringkat
- Acute AppendicitisDokumen9 halamanAcute AppendicitisSyarafina AzmanBelum ada peringkat
- Abdominal TBCDokumen11 halamanAbdominal TBCNitin SainiBelum ada peringkat
- Isi FixDokumen23 halamanIsi FixtarocikiBelum ada peringkat
- Endoscopy in Gastrointestinal TuberculosisDokumen6 halamanEndoscopy in Gastrointestinal TuberculosisChristine BelindaBelum ada peringkat
- Patho 9 JwanaDokumen19 halamanPatho 9 JwanajwanaBelum ada peringkat
- Inflammatory Bowel Disease Intestinal Obstruction and PolypsDokumen55 halamanInflammatory Bowel Disease Intestinal Obstruction and PolypsLiza Marie IgnacioBelum ada peringkat
- Abdominal TuberculosisDokumen9 halamanAbdominal TuberculosisImmanuelBelum ada peringkat
- Bab IDokumen31 halamanBab IAnonymous dv5AozsLBelum ada peringkat
- Which May Be Bloody If Inflammation Is Severe) : (I.e. Full Thickness of Bowel Wall)Dokumen4 halamanWhich May Be Bloody If Inflammation Is Severe) : (I.e. Full Thickness of Bowel Wall)abdullah albayatiBelum ada peringkat
- Diseases of Digestive SystemDokumen126 halamanDiseases of Digestive SystemKw ChanBelum ada peringkat
- The Vermiform Appendix: AnatomyDokumen10 halamanThe Vermiform Appendix: AnatomyBereket temesgenBelum ada peringkat
- Abdomen Clinical Review From KLM: 1.liposuctionDokumen11 halamanAbdomen Clinical Review From KLM: 1.liposuctionUsama SadiqBelum ada peringkat
- Case Study AppendicitisDokumen6 halamanCase Study AppendicitisPrincess Camille ArceoBelum ada peringkat
- GIT Pathology (Practical)Dokumen47 halamanGIT Pathology (Practical)jwan ahmedBelum ada peringkat
- The Vermiform AppendixDokumen17 halamanThe Vermiform AppendixSudhanshu ShekharBelum ada peringkat
- The Small Intestine and Colon Account For The Majority of GIDokumen13 halamanThe Small Intestine and Colon Account For The Majority of GIMohammed Yousif AbdualjabbarBelum ada peringkat
- Git PathologyDokumen113 halamanGit PathologyanggitaBelum ada peringkat
- 2 Semester 1 Major Patho AnatoDokumen49 halaman2 Semester 1 Major Patho AnatoManushi HenadeeraBelum ada peringkat
- Giant Appendiceal Mucocele: Report of A Case and Brief ReviewDokumen3 halamanGiant Appendiceal Mucocele: Report of A Case and Brief ReviewjulietBelum ada peringkat
- Lecture 23 - Gastrointestinal Tract - Part 2 - Clinical CorrelatesDokumen36 halamanLecture 23 - Gastrointestinal Tract - Part 2 - Clinical Correlatesspitzmark2030Belum ada peringkat
- Ulcer of The Stomac3Dokumen4 halamanUlcer of The Stomac3Ashucool65Belum ada peringkat
- Small Intestine and ColonDokumen9 halamanSmall Intestine and Colonlentini@maltanet.netBelum ada peringkat
- Gastro02 IntroGIPathDokumen6 halamanGastro02 IntroGIPathPatricia RuizBelum ada peringkat
- GIT - Lec. 2 DR - BasimDokumen28 halamanGIT - Lec. 2 DR - BasimEMIRZA NUR WICAKSONOBelum ada peringkat
- Ulcerative Colitis: Pathogenesis & PathologyDokumen12 halamanUlcerative Colitis: Pathogenesis & PathologyironBelum ada peringkat
- Ospe 4TH Year MBBS Exam Git ModuleDokumen45 halamanOspe 4TH Year MBBS Exam Git ModuleTahaBelum ada peringkat
- Anatomy Atresia, Volvulus, Meckel's Diverticulum: BowelDokumen45 halamanAnatomy Atresia, Volvulus, Meckel's Diverticulum: BowelkedokterankeluargaBelum ada peringkat
- Small and Large IntestinesDokumen44 halamanSmall and Large IntestinespempuladesmondsimfukwelBelum ada peringkat
- Summary For Acute AppendicitisDokumen13 halamanSummary For Acute AppendicitisFemale calmBelum ada peringkat
- Bab Ii Tinjauan Pustaka: 2.1 Anatomi Dan Fisiologi ApendiksDokumen18 halamanBab Ii Tinjauan Pustaka: 2.1 Anatomi Dan Fisiologi ApendiksFrischa TrirosaliaBelum ada peringkat
- Ulcerative ColitisDokumen88 halamanUlcerative ColitisYulia DjatiwardaniBelum ada peringkat
- Appendicitis: Made By: Madhurpreet KaurDokumen46 halamanAppendicitis: Made By: Madhurpreet KaurRAJAT DUGGALBelum ada peringkat
- Imaging in Inflammatory Bowel DiseaseDokumen38 halamanImaging in Inflammatory Bowel DiseaseIqbalAmriFauzalBelum ada peringkat
- Appendicitis InfiltratesDokumen14 halamanAppendicitis InfiltratesRiza Rahmalia100% (1)
- Abdomen-Clinicals - PDF Version 1Dokumen11 halamanAbdomen-Clinicals - PDF Version 1hamzabhayatBelum ada peringkat
- 1 ESOPHAGUS AND STOMACH - LearnDokumen119 halaman1 ESOPHAGUS AND STOMACH - LearnDavid KramerBelum ada peringkat
- 12 - Paediatric Abdomen RadiologyDokumen74 halaman12 - Paediatric Abdomen RadiologyMaria DoukaBelum ada peringkat
- Inflammatory Bowel DiseaseDokumen29 halamanInflammatory Bowel Diseasepriya madhooliBelum ada peringkat
- Acute Appendicitis in Adults Clinical Ma PDFDokumen27 halamanAcute Appendicitis in Adults Clinical Ma PDFAntonio Zumaque CarrascalBelum ada peringkat
- Etiology: Acute AppendicitisDokumen3 halamanEtiology: Acute AppendicitisWenna Grace OdtujanBelum ada peringkat
- (Lab) Patología II - Esófago y EstómagoDokumen82 halaman(Lab) Patología II - Esófago y EstómagoUSMP FN ARCHIVOSBelum ada peringkat
- Abdominal TuberculosisDokumen12 halamanAbdominal TuberculosisBimlesh ThakurBelum ada peringkat
- Appendicitis: Dr. Aplin I, SPBDokumen12 halamanAppendicitis: Dr. Aplin I, SPBAyu Kusuma NingrumBelum ada peringkat
- Background: Pediatric AppendicitisDokumen15 halamanBackground: Pediatric AppendicitisnikkitaihsanBelum ada peringkat
- Characteristics Ulcerative Colitis Crohn's DZDokumen2 halamanCharacteristics Ulcerative Colitis Crohn's DZIM CTBelum ada peringkat
- Acute PeritonitisDokumen11 halamanAcute Peritonitisangelmd83100% (1)
- Acute Appendicitis in Adults: Clinical Manifestations and DiagnosisDokumen37 halamanAcute Appendicitis in Adults: Clinical Manifestations and DiagnosisDaniela MuñozBelum ada peringkat
- Acute Appendicitis Pathophysiology: MycobacteriaDokumen10 halamanAcute Appendicitis Pathophysiology: MycobacteriaUzma KhanBelum ada peringkat
- Oil and Natural Gas Corporation Limited Western Offshore Unit, MumbaiDokumen6 halamanOil and Natural Gas Corporation Limited Western Offshore Unit, Mumbaisarath chandBelum ada peringkat
- QwertyDokumen3 halamanQwertysarath chandBelum ada peringkat
- QwertyDokumen3 halamanQwertysarath chandBelum ada peringkat
- The Greatest Muhammad Ali Book Common by Walter Dean by Author MyersDokumen6 halamanThe Greatest Muhammad Ali Book Common by Walter Dean by Author Myerssarath chandBelum ada peringkat
- Virus ShapesDokumen2 halamanVirus Shapessarath chandBelum ada peringkat
- מצגת מערכת עיכולDokumen74 halamanמצגת מערכת עיכולnataliya36Belum ada peringkat
- Gastroesophageal Reflux Disease - RepairedDokumen40 halamanGastroesophageal Reflux Disease - RepairedSowndharyaBelum ada peringkat
- Esophagus CAP ProtocolDokumen12 halamanEsophagus CAP ProtocolMichael Herman ChuiBelum ada peringkat
- Dyspepsia FinalDokumen52 halamanDyspepsia FinalAfifah SelamatBelum ada peringkat
- Utmb Absite Review ManualDokumen245 halamanUtmb Absite Review ManualEl Gonzo100% (1)
- GI Practice Review - 2nd Edition - ABRThomson 2012Dokumen744 halamanGI Practice Review - 2nd Edition - ABRThomson 2012Sultan AlexandruBelum ada peringkat
- MarchDokumen467 halamanMarchMike GreenBelum ada peringkat
- Esophegeal CancerDokumen32 halamanEsophegeal CancerShoaib HashmiBelum ada peringkat
- Barrett 'S EsophagusDokumen3 halamanBarrett 'S EsophagusI'Jaz Farritz MuhammadBelum ada peringkat
- 2017 - Alcohol, Smoking and Risk of Esophago-Gastric CancerDokumen9 halaman2017 - Alcohol, Smoking and Risk of Esophago-Gastric CancerPatricia Peñaflor GrimaldoBelum ada peringkat
- Endoscopic Submucosal Dissection: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineDokumen26 halamanEndoscopic Submucosal Dissection: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineMadalina StoicescuBelum ada peringkat
- Fundamentals of Pathology PathomaDokumen215 halamanFundamentals of Pathology Pathomaprachi jainBelum ada peringkat
- GI Internal Medicine PDFDokumen9 halamanGI Internal Medicine PDFArianneJulienaCervaniaAndradaBelum ada peringkat
- GerdDokumen51 halamanGerdaddfre100% (1)
- Asge BarretDokumen27 halamanAsge BarretIngrid González EfronBelum ada peringkat
- Gastroenterology Clinical Focus High Yield Gi and HepatologyDokumen426 halamanGastroenterology Clinical Focus High Yield Gi and HepatologyAhana MukherjeeBelum ada peringkat
- Barrett's Esophagus A Pathologist's ViewDokumen12 halamanBarrett's Esophagus A Pathologist's ViewRonnie Reyes MartínezBelum ada peringkat
- Surgery Part 3Dokumen8 halamanSurgery Part 3Jam JamaBelum ada peringkat
- Gastro Hepato ProgramDokumen56 halamanGastro Hepato ProgramGastro-Hepato 2022Belum ada peringkat
- Gastro 4Dokumen537 halamanGastro 4Andrei ManeaBelum ada peringkat
- GERDDokumen17 halamanGERDMafe Cabiles0% (1)
- 07a. Non Neoplastic Disease of OesophagusDokumen35 halaman07a. Non Neoplastic Disease of Oesophagus21701101016 - Juliana Ayu NugrahaBelum ada peringkat
- Gastroesophageal Reflux DiseaseDokumen11 halamanGastroesophageal Reflux DiseaseMike GBelum ada peringkat
- Master Radiology Notes GIT PDFDokumen115 halamanMaster Radiology Notes GIT PDFuroshkgBelum ada peringkat
- 3B CTC08 Gerd 10.01.16Dokumen41 halaman3B CTC08 Gerd 10.01.16Adriel PizarraBelum ada peringkat
- Barretts EsophagusDokumen21 halamanBarretts EsophagusLyka DimayacyacBelum ada peringkat
- Barret's Syndrome Case ReportDokumen3 halamanBarret's Syndrome Case ReportResearch ParkBelum ada peringkat
- GERD Definition, Patho and TreatmentDokumen7 halamanGERD Definition, Patho and TreatmentGeethika GummadiBelum ada peringkat
- Ajg2009492 1aDokumen40 halamanAjg2009492 1aseb2008Belum ada peringkat
- Internal Medicine (Internal Medicine) Merged PDFDokumen169 halamanInternal Medicine (Internal Medicine) Merged PDFHimanshuBelum ada peringkat