Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Basic Life SupportDokumen29 halamanBasic Life SupportRyan-Jay Abolencia100% (1)
- BHD - BIAK (PPT DR - Liza)Dokumen31 halamanBHD - BIAK (PPT DR - Liza)Vherty Vhertozt VuaztBelum ada peringkat
- Gunakan jari telunjuk dan jari tengah untuk membersihkan mulut dari benda asing. Jangan gunakan tangan utuh untuk membersihkan mulutDokumen81 halamanGunakan jari telunjuk dan jari tengah untuk membersihkan mulut dari benda asing. Jangan gunakan tangan utuh untuk membersihkan mulutBoby GeaBelum ada peringkat
- Glaucoma Surgery Guide: Trabeculectomy Complications & ManagementDokumen38 halamanGlaucoma Surgery Guide: Trabeculectomy Complications & ManagementGlaucoma UnhasBelum ada peringkat
- ERC BLS & AED Course: Learn Life-Saving SkillsDokumen34 halamanERC BLS & AED Course: Learn Life-Saving SkillsNicoleta Pîrju100% (1)
- Dasar Biomolekuler Reproduksi Pria: Kuliah 2Dokumen25 halamanDasar Biomolekuler Reproduksi Pria: Kuliah 2FitriaBelum ada peringkat
- Dasar Biomolekuler Reproduksi Pria: Kuliah 2Dokumen25 halamanDasar Biomolekuler Reproduksi Pria: Kuliah 2FitriaBelum ada peringkat
- A Metasynthesis of Midwives Experience oDokumen21 halamanA Metasynthesis of Midwives Experience oFitriaBelum ada peringkat
- Dasar2 Biomolekuler Repro WanitaDokumen51 halamanDasar2 Biomolekuler Repro WanitaFitriaBelum ada peringkat
- g1 PDFDokumen7 halamang1 PDFFitriaBelum ada peringkat
- Optimisme Kesembuhan Pada Penderita Mioma UteriDokumen13 halamanOptimisme Kesembuhan Pada Penderita Mioma UteriSyah DiyahBelum ada peringkat
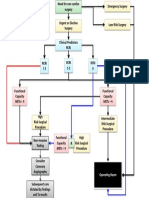
- Cardiac Risk Assessemnt FlowchartDokumen1 halamanCardiac Risk Assessemnt FlowchartjamesomooreBelum ada peringkat
- Peritoneal Dialysis Catheter Placement TechniquesDokumen2 halamanPeritoneal Dialysis Catheter Placement TechniquestitoBelum ada peringkat
- MAP Application Form (Rev20230719)Dokumen3 halamanMAP Application Form (Rev20230719)Jen EugenioBelum ada peringkat
- Tatalaksana KegawatdaruratanDokumen9 halamanTatalaksana KegawatdaruratanBennyBelum ada peringkat
- QUIZ Classification of Surgery in TableDokumen1 halamanQUIZ Classification of Surgery in TableMaria Sheila BelzaBelum ada peringkat
- List of EctomiesDokumen6 halamanList of EctomiesSatish PasulaBelum ada peringkat
- Ambulatory Hysteroscopy - Creating Certainty: The Solution For Diagnostics and Treatment in An Ambulatory SettingDokumen2 halamanAmbulatory Hysteroscopy - Creating Certainty: The Solution For Diagnostics and Treatment in An Ambulatory Settingreta.rose92Belum ada peringkat
- Sr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesDokumen49 halamanSr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesADDECC INFO INDIABelum ada peringkat
- Poster BLS AutomatedExternal Algorithm ENG V20151005 HRES SiteDokumen1 halamanPoster BLS AutomatedExternal Algorithm ENG V20151005 HRES SiteBryanCardenasBelum ada peringkat
- JANUARY 2019 PATIENT ANTIBIOTIC DATADokumen25 halamanJANUARY 2019 PATIENT ANTIBIOTIC DATAMaria AmabiBelum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar PustakaMustika TykaBelum ada peringkat
- European Resuscitation Council BLS GuideDokumen42 halamanEuropean Resuscitation Council BLS GuideNiken Tri HapsariBelum ada peringkat
- Endotracheal Tube ETT Insertion IntubationDokumen3 halamanEndotracheal Tube ETT Insertion IntubationmochkurniawanBelum ada peringkat
- Cosmetic Surgery in Manchester by Dr. Deemesh Oudit PDFDokumen5 halamanCosmetic Surgery in Manchester by Dr. Deemesh Oudit PDFDeemesh ouditBelum ada peringkat
- 08 - Privileges - General SurgeryDokumen3 halaman08 - Privileges - General SurgeryAccreditation ConsultantBelum ada peringkat
- Diagnosa Dan Tatalaksana Pada Hemoroid Derajat IV: Laporan KasusDokumen4 halamanDiagnosa Dan Tatalaksana Pada Hemoroid Derajat IV: Laporan KasusFajri AkhmadBelum ada peringkat
- Sleeve-Gastrectomy 2011 BrethauerDokumen15 halamanSleeve-Gastrectomy 2011 BrethauerDavid Schnettler RodriguezBelum ada peringkat
- Angioplasty and Stenting For Peripheral Arterial Disease of The Lower LimbsDokumen13 halamanAngioplasty and Stenting For Peripheral Arterial Disease of The Lower Limbsnadia shabriBelum ada peringkat
- Angiografi Femoralis-1Dokumen24 halamanAngiografi Femoralis-1Sepahit Kopi Hitam100% (1)
- Cataract: Classsification Acquired Age Related Nuclear Cortical Posterior Sub-CapsularDokumen37 halamanCataract: Classsification Acquired Age Related Nuclear Cortical Posterior Sub-CapsularBushra SherwaniBelum ada peringkat
- RDC 3385 Resolution Economic InfoDokumen4 halamanRDC 3385 Resolution Economic InfoLackner MarceloBelum ada peringkat
- Or Instruments 1Dokumen55 halamanOr Instruments 1Stephanie LeeBelum ada peringkat
- India Live 2019 - Case Submission Result: S.No Name Category Case NameDokumen9 halamanIndia Live 2019 - Case Submission Result: S.No Name Category Case NameRajendra ChavanBelum ada peringkat
- Orthopaedic Fellowships in India After PGDokumen4 halamanOrthopaedic Fellowships in India After PGNEPDOC OFFICIAL100% (1)
- Clear Trac CompDokumen2 halamanClear Trac Compapi-19808945Belum ada peringkat