Anda mungkin juga menyukai
- Atm 08 20 1292Dokumen11 halamanAtm 08 20 1292Ethel GeanBelum ada peringkat
- J Amjoto 2019 102279Dokumen5 halamanJ Amjoto 2019 102279Gisela LalitaBelum ada peringkat
- Improved Outcome by Adding Concurrent Chemotherapy ToDokumen9 halamanImproved Outcome by Adding Concurrent Chemotherapy ToRaul Matute MartinBelum ada peringkat
- PIIS0003497509010868Dokumen6 halamanPIIS0003497509010868Karthik SgBelum ada peringkat
- Radiotherapy and OncologyDokumen6 halamanRadiotherapy and OncologyIntan Kartika NursyahbaniBelum ada peringkat
- Staging Lung CancerDokumen20 halamanStaging Lung Cancerrohil jainBelum ada peringkat
- Jurnal Radiologi 2Dokumen21 halamanJurnal Radiologi 2Adelya Dwi AsyifaBelum ada peringkat
- Delineating Organs at Risk in Radiation TherapyDari EverandDelineating Organs at Risk in Radiation TherapyBelum ada peringkat
- Rcsann 2016 0300Dokumen4 halamanRcsann 2016 0300Siti Ayu kamsiahBelum ada peringkat
- Lynch Syndrome: Molecular Mechanism and Current Clinical PracticeDari EverandLynch Syndrome: Molecular Mechanism and Current Clinical PracticeNaohiro TomitaBelum ada peringkat
- Hypofractionated and Stereotactic Radiation Therapy: A Practical GuideDari EverandHypofractionated and Stereotactic Radiation Therapy: A Practical GuideOrit Kaidar-PersonBelum ada peringkat
- Metastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyDokumen6 halamanMetastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyMara PitrezBelum ada peringkat
- Surgical Treatment of Trichilemmal CarcinomaDokumen4 halamanSurgical Treatment of Trichilemmal CarcinomaNESRINE MARZAKBelum ada peringkat
- Contemporary Approach To The Diagnosis of Malignant Pleural EffusionDokumen8 halamanContemporary Approach To The Diagnosis of Malignant Pleural EffusionranityaindraBelum ada peringkat
- DTH 34 E14981Dokumen9 halamanDTH 34 E14981Henry WijayaBelum ada peringkat
- Endoscopic Management of Colorectal T1(SM) CarcinomaDari EverandEndoscopic Management of Colorectal T1(SM) CarcinomaShinji TanakaBelum ada peringkat
- 3.MRI of HCCDokumen13 halaman3.MRI of HCCOana AndreeaBelum ada peringkat
- Radiol 2018180979Dokumen9 halamanRadiol 2018180979Aze Andrea PutraBelum ada peringkat
- 2019 Article 5894 PDFDokumen8 halaman2019 Article 5894 PDFGalgalo GarbichaBelum ada peringkat
- J Joms 2016 03 037Dokumen12 halamanJ Joms 2016 03 037Gisela LalitaBelum ada peringkat
- JTD 09 03 768Dokumen11 halamanJTD 09 03 768nanaBelum ada peringkat
- 2012 - Yoon Et Al. - Contouring Guidelines of The Inguinal Lymph Nodes Using Lymphangiograms For The Delivery of Radiation Therapy in GastroDokumen1 halaman2012 - Yoon Et Al. - Contouring Guidelines of The Inguinal Lymph Nodes Using Lymphangiograms For The Delivery of Radiation Therapy in GastroPoljarLijanBelum ada peringkat
- AtomDokumen13 halamanAtomapi-3821924Belum ada peringkat
- File 1Dokumen4 halamanFile 1Marsya Yulinesia LoppiesBelum ada peringkat
- Hallifax Radiological Investigation of Pleural DiseaseDokumen38 halamanHallifax Radiological Investigation of Pleural Diseaselaila.forestaBelum ada peringkat
- 1 s2.0 S1556086415306973 MainDokumen8 halaman1 s2.0 S1556086415306973 MainLaura QuirozBelum ada peringkat
- F-FDG PET CT As A Prognostic Factor in Hepatocellular CarcinomaDokumen7 halamanF-FDG PET CT As A Prognostic Factor in Hepatocellular CarcinomaUvi Cancino RamosBelum ada peringkat
- Jurnal Patologi AnatomiDokumen5 halamanJurnal Patologi Anatomiafiqzakieilhami11Belum ada peringkat
- 11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayDokumen8 halaman11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayBridia BogarBelum ada peringkat
- Lung Cancer Current Therapies and New Targeted TreatmentsDokumen13 halamanLung Cancer Current Therapies and New Targeted TreatmentsWlad PaCaBelum ada peringkat
- Management of The Solitary Pulmonary NoduleDokumen6 halamanManagement of The Solitary Pulmonary Nodulevictor ibarra romeroBelum ada peringkat
- Clinicopathological Predictors of Central Compartment Lymph Node Metastases in cN0 Papillary Thyroid CarcinomaDokumen11 halamanClinicopathological Predictors of Central Compartment Lymph Node Metastases in cN0 Papillary Thyroid CarcinomaYacine Tarik AizelBelum ada peringkat
- Seminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresDokumen13 halamanSeminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresseruniallisaaslimBelum ada peringkat
- Current Concepts in The Diagnosis and Staging of Lung CancerDokumen15 halamanCurrent Concepts in The Diagnosis and Staging of Lung CancerVictor ChiabaiBelum ada peringkat
- Critical Changes in The Staging of Head and Neck Cancer: Christine M. Glastonbury, MBBSDokumen8 halamanCritical Changes in The Staging of Head and Neck Cancer: Christine M. Glastonbury, MBBSEMIRZA NUR WICAKSONOBelum ada peringkat
- Glimelius 2013Dokumen8 halamanGlimelius 2013Sofia SimpertigueBelum ada peringkat
- Pet CT and Pet Mri in Head and Neck MalignancyDokumen10 halamanPet CT and Pet Mri in Head and Neck MalignancyAndrés Faúndez TeránBelum ada peringkat
- MainDokumen8 halamanMainNurulrezki AtikaBelum ada peringkat
- Tumor Liquid BiopsiesDari EverandTumor Liquid BiopsiesFlorence SchaffnerBelum ada peringkat
- Esmo Clinical GuidelinesDokumen3 halamanEsmo Clinical GuidelinesAbdi Hakin MohamedBelum ada peringkat
- Ashworth 2013Dokumen7 halamanAshworth 2013Laura QuirozBelum ada peringkat
- Imaging in Peripheral Arterial Disease: Clinical and Research ApplicationsDari EverandImaging in Peripheral Arterial Disease: Clinical and Research ApplicationsBelum ada peringkat
- Clinical Practice GuidelinesDokumen7 halamanClinical Practice GuidelinesRoppeBelum ada peringkat
- The Prognostic Significance of Tall Cells in Papillary Thyroid Carcinoma: A Case-Control StudyDokumen7 halamanThe Prognostic Significance of Tall Cells in Papillary Thyroid Carcinoma: A Case-Control StudyHula HulahulagBelum ada peringkat
- CA MammaeDokumen6 halamanCA MammaeRiaBelum ada peringkat
- A Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerDokumen9 halamanA Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerFarizka Dwinda HBelum ada peringkat
- Vera2020 Article MultidisciplinaryManagementOfLDokumen16 halamanVera2020 Article MultidisciplinaryManagementOfLDiego Andres VasquezBelum ada peringkat
- 2016 Article 826Dokumen6 halaman2016 Article 826tomniucBelum ada peringkat
- Referensi 1Dokumen9 halamanReferensi 1Indah Syaidatul MBelum ada peringkat
- Role of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomaDokumen8 halamanRole of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomadickyaririsandyBelum ada peringkat
- The Laryngoscope - 2020 - Vincent - Treatment of Oligometastatic Disease in Squamous Cell Carcinoma of The Head and Neck PDFDokumen5 halamanThe Laryngoscope - 2020 - Vincent - Treatment of Oligometastatic Disease in Squamous Cell Carcinoma of The Head and Neck PDFanoop_aiims1Belum ada peringkat
- PublishedDokumen5 halamanPublishedMudassar SaeedBelum ada peringkat
- Total Marrow Irradiation: A Comprehensive ReviewDari EverandTotal Marrow Irradiation: A Comprehensive ReviewJeffrey Y. C. WongBelum ada peringkat
- Lung SOL - Cytology and Histological Correlation in A Tertiary Care CentreDokumen7 halamanLung SOL - Cytology and Histological Correlation in A Tertiary Care CentreIOSRjournalBelum ada peringkat
- Theraphy RadDokumen4 halamanTheraphy RadMega PuspitaBelum ada peringkat
- 10 1053@j Semnuclmed 2020 07 005Dokumen10 halaman10 1053@j Semnuclmed 2020 07 005anon_813722240Belum ada peringkat
- P1337430319048 - Artikel Jurnal 1Dokumen6 halamanP1337430319048 - Artikel Jurnal 1maulanagam69Belum ada peringkat
- Behranwala 2003Dokumen11 halamanBehranwala 2003Therese Justine BruelBelum ada peringkat
- Piis0167814019331123 230304 134522Dokumen7 halamanPiis0167814019331123 230304 134522Samuel Kelvin RuslimBelum ada peringkat
- Predictive Value of Nodal Metastases On Local Recurrence in The Management of Differentiated Thyroid Cancer. Retrospective Clinical StudyDokumen6 halamanPredictive Value of Nodal Metastases On Local Recurrence in The Management of Differentiated Thyroid Cancer. Retrospective Clinical StudyuqbaBelum ada peringkat
- ADokumen1 halamanAjosBelum ada peringkat
- Reporte Viga ADokumen15 halamanReporte Viga AjosBelum ada peringkat
- Areas VirgilioDokumen2 halamanAreas VirgiliojosBelum ada peringkat
- Seccion DannyDokumen7 halamanSeccion DannyjosBelum ada peringkat
- Informacion TopograficaDokumen5 halamanInformacion TopograficajosBelum ada peringkat
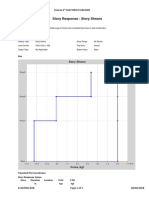
- Story Response - Story Shears: ETABS 2016 16.2.0 License # 1Z8VYN5FWWBEHHNDokumen2 halamanStory Response - Story Shears: ETABS 2016 16.2.0 License # 1Z8VYN5FWWBEHHNjosBelum ada peringkat
- Filtros de Arena-PlantaDokumen1 halamanFiltros de Arena-PlantajosBelum ada peringkat
- You Created This PDF From An Application That Is Not Licensed To Print To Novapdf PrinterDokumen1 halamanYou Created This PDF From An Application That Is Not Licensed To Print To Novapdf PrinterjosBelum ada peringkat
- Virani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdateDokumen490 halamanVirani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdatehendridunantikoBelum ada peringkat
- NSG ProcessDokumen6 halamanNSG ProcessJay-Dee Evangelista PacionBelum ada peringkat
- Epidemiology of Sarcopenia Prevalence, Risk FactoDokumen9 halamanEpidemiology of Sarcopenia Prevalence, Risk FactoW Antonio Rivera MartínezBelum ada peringkat
- Mirikizumab As Induction and Maintenance Therapy For UlcerativeDokumen15 halamanMirikizumab As Induction and Maintenance Therapy For Ulcerativesreebhahun satishBelum ada peringkat
- KalingaDLL-scientific Literacy & Critical ThinkingDokumen4 halamanKalingaDLL-scientific Literacy & Critical ThinkingMary Joy Lucob TangbawanBelum ada peringkat
- HemostasisDokumen5 halamanHemostasisPadmavathi C100% (1)
- Touch Imprint Cytology: A Rapid and Accurate Method For Diagnosis of Oral Cancer Original ArticleDokumen19 halamanTouch Imprint Cytology: A Rapid and Accurate Method For Diagnosis of Oral Cancer Original ArticleNiketa SharmaBelum ada peringkat
- Medication Administration Nursing PracticeDokumen34 halamanMedication Administration Nursing PracticeSWATBelum ada peringkat
- Poster Urine Sediment - GBDokumen1 halamanPoster Urine Sediment - GBROBERTO CESPEDES0% (1)
- Sophia Guy ResumeDokumen3 halamanSophia Guy Resumeapi-677670066Belum ada peringkat
- XN-1500 10p ENDokumen5 halamanXN-1500 10p ENHarika PutraBelum ada peringkat
- Mock Ospe Me211Dokumen15 halamanMock Ospe Me211sahirbuleBelum ada peringkat
- Final Osce Care PlanDokumen8 halamanFinal Osce Care Planapi-526590140100% (1)
- TWSTRS Severity ScaleDokumen2 halamanTWSTRS Severity ScaleErri PratamaBelum ada peringkat
- Drug Study FluimucilDokumen2 halamanDrug Study FluimucilJemina Rafanan Racadio0% (1)
- Ortho Referral Quick Reference SheetDokumen2 halamanOrtho Referral Quick Reference SheetAbdelhamid FaragBelum ada peringkat
- Fadila Kemala Dwi Ramadhani Ruslan - Revisi Kbpji 2Dokumen16 halamanFadila Kemala Dwi Ramadhani Ruslan - Revisi Kbpji 2Eugenia RussiavBelum ada peringkat
- Clinician - S Guide To Sleep Disorders (Watson - Vaughn, 2006) PDFDokumen411 halamanClinician - S Guide To Sleep Disorders (Watson - Vaughn, 2006) PDFMarta PamolBelum ada peringkat
- Barodontalgia As A Differential Diagnosis PDFDokumen4 halamanBarodontalgia As A Differential Diagnosis PDFDavid ColonBelum ada peringkat
- National Integrated Emergency Medicine TrainingDokumen274 halamanNational Integrated Emergency Medicine TrainingAddisu AdaneBelum ada peringkat
- Vaccines and Vaccination History and Emerging IssuesDokumen15 halamanVaccines and Vaccination History and Emerging IssuesMěđ SimoBelum ada peringkat
- BPH First Year Curriculum of Purbanchal UniversityDokumen48 halamanBPH First Year Curriculum of Purbanchal Universityseo167Belum ada peringkat
- The Role of Acute Phase Proteins in Diagnosis and ManagementDokumen6 halamanThe Role of Acute Phase Proteins in Diagnosis and ManagementCabinet VeterinarBelum ada peringkat
- Reviewer RenalDokumen13 halamanReviewer Renalsean blaze100% (1)
- 2014 09 - LOINC Tutorial - ImagingDokumen34 halaman2014 09 - LOINC Tutorial - ImagingDaniel VreemanBelum ada peringkat
- Dams Video Based TestDokumen30 halamanDams Video Based TestPandey AyushBelum ada peringkat
- Ketogenic DietDokumen8 halamanKetogenic DietzabedahibrahimBelum ada peringkat
- Fetal Distress Day 1Dokumen16 halamanFetal Distress Day 1day dayu100% (1)
- AsplDokumen9 halamanAsplCristinaBelum ada peringkat
- Magnesium Sulfat: Maisuri T. ChalidDokumen23 halamanMagnesium Sulfat: Maisuri T. ChalidDevy Oktavia AnisaBelum ada peringkat