Anda mungkin juga menyukai
- Basic Exercise Physiology: Clinical and Laboratory PerspectivesDari EverandBasic Exercise Physiology: Clinical and Laboratory PerspectivesBelum ada peringkat
- Trunk Muscle EMG During Intermediate Pilates Mat Exercises in Beginner Healthy and Chronic Low Back Pain IndividualsDokumen8 halamanTrunk Muscle EMG During Intermediate Pilates Mat Exercises in Beginner Healthy and Chronic Low Back Pain IndividualsDiana Magnavita MouraBelum ada peringkat
- Artigo Afundo 2Dokumen8 halamanArtigo Afundo 2Yan MatosBelum ada peringkat
- PNF Training Improves Back Pain and FunctionDokumen12 halamanPNF Training Improves Back Pain and FunctionEdo Orlando Galicia PinazoBelum ada peringkat
- Muscle Activation During Exercises To Improve TrunkDokumen9 halamanMuscle Activation During Exercises To Improve TrunkYoh ChenBelum ada peringkat
- O'Sullivan Posture Muscle Activity 02Dokumen7 halamanO'Sullivan Posture Muscle Activity 02Hugo ArezBelum ada peringkat
- High Load Lifting Exercise and Low Load Motor Control Exercises As Interventions For Patients With Mechanical Low Back Pain: A Randomized Controlled Trial With 24-Month Follow-UpDokumen8 halamanHigh Load Lifting Exercise and Low Load Motor Control Exercises As Interventions For Patients With Mechanical Low Back Pain: A Randomized Controlled Trial With 24-Month Follow-UpbellaBelum ada peringkat
- Rossi2014 PDFDokumen8 halamanRossi2014 PDFDiana Magnavita MouraBelum ada peringkat
- Ijerph 16 03509Dokumen11 halamanIjerph 16 03509Chloe BujuoirBelum ada peringkat
- The Influence of An Unstable Surface On Trunk and Lower Extremity Muscle Activities During Variable Bridging ExercisesDokumen3 halamanThe Influence of An Unstable Surface On Trunk and Lower Extremity Muscle Activities During Variable Bridging ExercisesSulvina IbrahimBelum ada peringkat
- Ultrasound Evaluation of The Abdominal Wall and Lumbar Multifidus Muscles in Participants Who Practice Pilates: A 1-Year Follow-Up Case SeriesDokumen11 halamanUltrasound Evaluation of The Abdominal Wall and Lumbar Multifidus Muscles in Participants Who Practice Pilates: A 1-Year Follow-Up Case SeriesDiana Magnavita MouraBelum ada peringkat
- Core Muscle Function During Specific Yoga PosesDokumen9 halamanCore Muscle Function During Specific Yoga PosesRafliBelum ada peringkat
- 1 s2.0 S0965229914000107 MainDokumen9 halaman1 s2.0 S0965229914000107 MainToàn Huu NguyenBelum ada peringkat
- Exercise Technique: The Long-Lever Posterior-Tilt PlankDokumen2 halamanExercise Technique: The Long-Lever Posterior-Tilt Plankdejvidveb1988Belum ada peringkat
- Effects of Stabilization Exercise Using Flexi-Bar OnDokumen5 halamanEffects of Stabilization Exercise Using Flexi-Bar OnYoh ChenBelum ada peringkat
- Effects of Respiratory-Muscle Exercise On Spinal CurvatureDokumen6 halamanEffects of Respiratory-Muscle Exercise On Spinal CurvatureChrisBelum ada peringkat
- 2020 Berckmans Finewire AJSMDokumen7 halaman2020 Berckmans Finewire AJSMMariaBelum ada peringkat
- 2020 Berckmans Finewire AJSMDokumen7 halaman2020 Berckmans Finewire AJSMLívia PogettiBelum ada peringkat
- HemiplejiaDokumen10 halamanHemiplejiaCamila Velasco RojasBelum ada peringkat
- Ithamar 2017Dokumen33 halamanIthamar 2017Einar Cumplido MartínezBelum ada peringkat
- 72-Article Text-135-1-10-20190522 PDFDokumen7 halaman72-Article Text-135-1-10-20190522 PDFestherBelum ada peringkat
- 72-Article Text-135-1-10-20190522 PDFDokumen7 halaman72-Article Text-135-1-10-20190522 PDFestherBelum ada peringkat
- 2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseDokumen23 halaman2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseFrancisco Antonó Castro WeithBelum ada peringkat
- Trunk Position Influences The Kinematics, Farrokhi 2008Dokumen7 halamanTrunk Position Influences The Kinematics, Farrokhi 2008Ronald MasisBelum ada peringkat
- Evidence of Altered Lumbopelvic Muscle Recruitment in The Presence of SI Joint Pain.Dokumen8 halamanEvidence of Altered Lumbopelvic Muscle Recruitment in The Presence of SI Joint Pain.Christian Donoso AguilarBelum ada peringkat
- Effect of Head and Limb Orientation On Trunk Muscle Activation During Abdominal Hollowing in Chronic Low Back PainDokumen12 halamanEffect of Head and Limb Orientation On Trunk Muscle Activation During Abdominal Hollowing in Chronic Low Back PainCathrine MyrlandBelum ada peringkat
- Electromyographic Analysis of Traditional and Non Traditional Abdominal ExercisesDokumen16 halamanElectromyographic Analysis of Traditional and Non Traditional Abdominal ExercisesRafael EscamillaBelum ada peringkat
- Brazilian Journal of Physical TherapyDokumen10 halamanBrazilian Journal of Physical TherapyLuis DavidBelum ada peringkat
- Lumbar Stability PDFDokumen9 halamanLumbar Stability PDFPablo EstebanBelum ada peringkat
- Robello_et_al_2021_Optimal_activation_ratio_of_the_scapular_musclesDokumen14 halamanRobello_et_al_2021_Optimal_activation_ratio_of_the_scapular_musclesLina M GarciaBelum ada peringkat
- Core Stability Exercise PrinciplesDokumen6 halamanCore Stability Exercise Principlesphysioali0% (2)
- Accepted: Laboratory of Electromyography and Orthopedics - UFVJMDokumen21 halamanAccepted: Laboratory of Electromyography and Orthopedics - UFVJMDiana Magnavita MouraBelum ada peringkat
- Importance of Mind-Muscle Connection During Progressive Resistance Training PDFDokumen7 halamanImportance of Mind-Muscle Connection During Progressive Resistance Training PDFcaioBelum ada peringkat
- Ctar Vs ShakerDokumen11 halamanCtar Vs Shakeralejandra perezBelum ada peringkat
- 10 1097@JWH 0000000000000102Dokumen11 halaman10 1097@JWH 0000000000000102Winda YaniBelum ada peringkat
- Differences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFDokumen3 halamanDifferences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFLeonardiniBelum ada peringkat
- 2007 Lumbar Stabilization Part 2 PDFDokumen9 halaman2007 Lumbar Stabilization Part 2 PDFPatricia Andrea Acevedo ArancibiaBelum ada peringkat
- Schenkman: Exercise To Improve Spinal Flexibility and Function For People With Parkinson's Disease: A Randomized, Controlled TrialDokumen10 halamanSchenkman: Exercise To Improve Spinal Flexibility and Function For People With Parkinson's Disease: A Randomized, Controlled TrialGerman BuyattiBelum ada peringkat
- BestDokumen3 halamanBestRitika JangraBelum ada peringkat
- Ativaçñao de GluteosDokumen4 halamanAtivaçñao de GluteosRafael SanchezBelum ada peringkat
- Neuromuscular Training in PFPS Protocol BMC 2014Dokumen10 halamanNeuromuscular Training in PFPS Protocol BMC 2014Michele GonçalvesBelum ada peringkat
- Rehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureDokumen4 halamanRehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureSAMBelum ada peringkat
- 23 247Dokumen4 halaman23 247Ita MagdalenaBelum ada peringkat
- Low Back Pain and Muscles ActivityDokumen7 halamanLow Back Pain and Muscles Activitycris.endo.ceBelum ada peringkat
- SciDokumen9 halamanSciCathyCarltonBelum ada peringkat
- 24 - JPTS 2012 156Dokumen4 halaman24 - JPTS 2012 156Βιβιλάκη ΓεωργίαBelum ada peringkat
- Trunk Muscle Activities During Abdominal Bracing: Comparison Among Muscles and ExercisesDokumen9 halamanTrunk Muscle Activities During Abdominal Bracing: Comparison Among Muscles and ExercisesSorin IonutBelum ada peringkat
- An ElectromyograpDokumen13 halamanAn ElectromyograpSara AguiarBelum ada peringkat
- Dolor Espalda 6Dokumen7 halamanDolor Espalda 6Pablo Ignacio Nova BaezaBelum ada peringkat
- Pilates RandomizadoDokumen13 halamanPilates RandomizadorodrigueuresBelum ada peringkat
- 10 3390@medicina57070702Dokumen7 halaman10 3390@medicina57070702Einar Cumplido MartínezBelum ada peringkat
- Reinold - Glenohumeral and Scapulothoracic RehabDokumen45 halamanReinold - Glenohumeral and Scapulothoracic Rehabshivnair100% (2)
- Willians EfectividsdDokumen7 halamanWillians EfectividsdOmar CeliBelum ada peringkat
- ScoliosesDokumen10 halamanScolioseschandiwalaBelum ada peringkat
- Interferencial em Cervicalgia EMG Jarcet 2011Dokumen9 halamanInterferencial em Cervicalgia EMG Jarcet 2011Michele GonçalvesBelum ada peringkat
- Title: Instructions For UseDokumen5 halamanTitle: Instructions For UseAnonymous b2k9ABe7eBelum ada peringkat
- Trunk Muscle Activity During Trunk Stabilizing Exercise With Isometric HipDokumen7 halamanTrunk Muscle Activity During Trunk Stabilizing Exercise With Isometric Hipjimelsanmartin447Belum ada peringkat
- O Efeito Agudo Do Exercício de Pilates Na Extremidade Inferior MáximaDokumen8 halamanO Efeito Agudo Do Exercício de Pilates Na Extremidade Inferior MáximaThiago SartiBelum ada peringkat
- Concurrent Aerobic and Strength Training: Scientific Basics and Practical ApplicationsDari EverandConcurrent Aerobic and Strength Training: Scientific Basics and Practical ApplicationsMoritz SchumannBelum ada peringkat
- Healthy Percentage Body Fat Ranges An Approach ForDokumen9 halamanHealthy Percentage Body Fat Ranges An Approach ForThe Fitness CoachBelum ada peringkat
- NCSF Personal Trainer Exam Candidate HandbookDokumen28 halamanNCSF Personal Trainer Exam Candidate HandbookThe Fitness CoachBelum ada peringkat
- Carbohydrates Boudreaux PDFDokumen31 halamanCarbohydrates Boudreaux PDFMae MatiasBelum ada peringkat
- Howe 2017Dokumen11 halamanHowe 2017The Fitness CoachBelum ada peringkat
- Ul - Flexor - Forearm PDFDokumen29 halamanUl - Flexor - Forearm PDFArchishma ArchuBelum ada peringkat
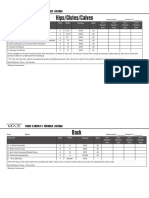
- Hips/Glutes/Calves: Phase 4/month 4 Workout JournalDokumen6 halamanHips/Glutes/Calves: Phase 4/month 4 Workout JournalDon SalhiBelum ada peringkat
- Thyroid DiseaseDokumen25 halamanThyroid DiseaseroserosannaBelum ada peringkat
- Ata Hypothyroidism BrochureDokumen3 halamanAta Hypothyroidism BrochureThe Fitness CoachBelum ada peringkat
- ACFT Instructions 1Dokumen31 halamanACFT Instructions 1jordonprice1114Belum ada peringkat
- AOFAS Ankle Hindfoot Scale.d5404138Dokumen1 halamanAOFAS Ankle Hindfoot Scale.d5404138yudiBelum ada peringkat
- Gyrokinesis Beginner Series Abs Back StretchesDokumen11 halamanGyrokinesis Beginner Series Abs Back StretchesSF Wong100% (2)
- Physical Therapy Protocols For Ankle and Foot ConditionsDokumen116 halamanPhysical Therapy Protocols For Ankle and Foot ConditionstinadasilvaBelum ada peringkat
- Eversion (Medial) Ankle Sprain: What It Is Immediate TreatmentDokumen2 halamanEversion (Medial) Ankle Sprain: What It Is Immediate TreatmentArrfanndi SeptianoBelum ada peringkat
- Pain Dan Kaku Leher Akibat Capsular Pattern Kasus SACDokumen10 halamanPain Dan Kaku Leher Akibat Capsular Pattern Kasus SACAfifah NurBelum ada peringkat
- Childhood IllnessDokumen32 halamanChildhood IllnessJesseBelum ada peringkat
- Yoga For Knee Pain 5 Poses To Add Strength & Reduce DiscomfortDokumen6 halamanYoga For Knee Pain 5 Poses To Add Strength & Reduce DiscomfortWazzah BieBelum ada peringkat
- Hip and FootDokumen14 halamanHip and FootKoj Lozada100% (1)
- The Biomechanical ModelDokumen17 halamanThe Biomechanical ModelLama NammouraBelum ada peringkat
- HUMAN BIOmuscles Origin Insertion ActionDokumen3 halamanHUMAN BIOmuscles Origin Insertion ActionandrealohrBelum ada peringkat
- Badminton BibleDokumen223 halamanBadminton BibleDanny Dawson50% (2)
- Movement Preparation ExercisesDokumen28 halamanMovement Preparation ExercisesCláudio Alves0% (1)
- AEPS Criteria Birth To 3Dokumen49 halamanAEPS Criteria Birth To 3Yamuna Govindaraj100% (1)
- Physio ExercisesDokumen11 halamanPhysio ExercisesRonak PatelBelum ada peringkat
- Bulmarc PU Ebook 2020 WebDokumen70 halamanBulmarc PU Ebook 2020 Webkshitij_gaur13100% (1)
- The Aerial Rope Manual: Rebekah LeachDokumen13 halamanThe Aerial Rope Manual: Rebekah LeachRemote Office100% (2)
- 03 Hand Rehabilitation of Stroke PatientsDokumen6 halaman03 Hand Rehabilitation of Stroke PatientsMd. Mizanur RahmanBelum ada peringkat
- Shoulder Adhesive Capsulitis ProtocolsDokumen3 halamanShoulder Adhesive Capsulitis ProtocolsAngelaBelum ada peringkat
- Ballard ScoreDokumen11 halamanBallard ScoreHoneylit YapBelum ada peringkat
- Above-Knee Prosthetics: The Knud Jansen LectureDokumen15 halamanAbove-Knee Prosthetics: The Knud Jansen LecturerkBelum ada peringkat
- Hip Mobility ExercisesDokumen1 halamanHip Mobility ExercisesT'om MoohtornBelum ada peringkat
- Body Mechanics and Patient CareDokumen79 halamanBody Mechanics and Patient CareChristian DioBelum ada peringkat
- Classification of Philippine DancesDokumen10 halamanClassification of Philippine DancesChristen Honely DadangBelum ada peringkat
- Wag - Cast in SupportDokumen2 halamanWag - Cast in Supportapi-443327549Belum ada peringkat
- Fundamentals of Hand Therapy Clinical Reasoning and Treatment Guidelines For Common Diagnoses of The Upper Extremity PDFDokumen561 halamanFundamentals of Hand Therapy Clinical Reasoning and Treatment Guidelines For Common Diagnoses of The Upper Extremity PDFDirk Gently100% (5)
- Glossary of Anatomical TerminologyDokumen3 halamanGlossary of Anatomical TerminologypoggerBelum ada peringkat
- UPPER LIMB - 6 Spinal Cord Segments, Dermatomes and Myotomes of The Upper LimbDokumen3 halamanUPPER LIMB - 6 Spinal Cord Segments, Dermatomes and Myotomes of The Upper LimbAbbas AliBelum ada peringkat
- Neck ROM Exercises Ver1 01.08.18Dokumen2 halamanNeck ROM Exercises Ver1 01.08.18kang soon cheolBelum ada peringkat
- Biometrics Goniometer UgDokumen24 halamanBiometrics Goniometer UgMohd Khairul Ikhwan AhmadBelum ada peringkat