Anda mungkin juga menyukai
- For Portfolio LS6 Digital CitizenshipDokumen4 halamanFor Portfolio LS6 Digital CitizenshipDon'tAsK TheStupidOnesBelum ada peringkat
- For Portfolio LS3 Mathematical and Problem Solving SkillsDokumen8 halamanFor Portfolio LS3 Mathematical and Problem Solving SkillsDon'tAsK TheStupidOnesBelum ada peringkat
- For Portfolio LS2 ScienceDokumen7 halamanFor Portfolio LS2 ScienceDon'tAsK TheStupidOnesBelum ada peringkat
- Crystal Structure Quiz: Name: - DateDokumen1 halamanCrystal Structure Quiz: Name: - DateDon'tAsK TheStupidOnesBelum ada peringkat
- Quiz 2 - ChemDokumen3 halamanQuiz 2 - ChemDon'tAsK TheStupidOnesBelum ada peringkat
- For Portfolio LS1 EnglishDokumen5 halamanFor Portfolio LS1 EnglishDon'tAsK TheStupidOnesBelum ada peringkat
- Welcome General Chemistry For Engineering and TechnologistDokumen9 halamanWelcome General Chemistry For Engineering and TechnologistDon'tAsK TheStupidOnesBelum ada peringkat
- Biology BasicsDokumen5 halamanBiology BasicsDon'tAsK TheStupidOnesBelum ada peringkat
- Principles of Biology I Lab ManualDokumen75 halamanPrinciples of Biology I Lab ManualDon'tAsK TheStupidOnesBelum ada peringkat
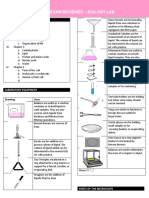
- Prelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Dokumen7 halamanPrelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Don'tAsK TheStupidOnesBelum ada peringkat
- Lesson 2 - Water, CarbohydratesDokumen22 halamanLesson 2 - Water, CarbohydratesDon'tAsK TheStupidOnesBelum ada peringkat
- Crystal Structure Quiz: Name: - DateDokumen1 halamanCrystal Structure Quiz: Name: - DateDon'tAsK TheStupidOnesBelum ada peringkat
- Hess's Law Problems SolvedDokumen2 halamanHess's Law Problems SolvedTjrjfjdjBelum ada peringkat
- Pathophysiology of TuberculosisDokumen1 halamanPathophysiology of TuberculosisDon'tAsK TheStupidOnesBelum ada peringkat
- Quiz 1-ChemDokumen2 halamanQuiz 1-ChemDon'tAsK TheStupidOnesBelum ada peringkat
- EF2017 FinalDigital PDFDokumen20 halamanEF2017 FinalDigital PDFHieuBelum ada peringkat
- Family Life Cycle StagesDokumen2 halamanFamily Life Cycle StagesDon'tAsK TheStupidOnes100% (1)
- Global Warming: Public Health Impacts and SolutionsDokumen45 halamanGlobal Warming: Public Health Impacts and SolutionsDon'tAsK TheStupidOnesBelum ada peringkat
- Bomb Calorimetry Practice ProblemsDokumen2 halamanBomb Calorimetry Practice ProblemsDon'tAsK TheStupidOnesBelum ada peringkat
- Gibbs WorksheetDokumen4 halamanGibbs WorksheetDon'tAsK TheStupidOnesBelum ada peringkat
- KEY Nuclear EquationsDokumen3 halamanKEY Nuclear EquationsDon'tAsK TheStupidOnesBelum ada peringkat
- Cross WordDokumen1 halamanCross WordDon'tAsK TheStupidOnesBelum ada peringkat
- Internal energy problems solutionsDokumen3 halamanInternal energy problems solutionsDon'tAsK TheStupidOnesBelum ada peringkat
- Comparison Between Piezoelectric and Magnetic PDFDokumen6 halamanComparison Between Piezoelectric and Magnetic PDFDon'tAsK TheStupidOnesBelum ada peringkat
- Calorimetry Problems KeyDokumen2 halamanCalorimetry Problems KeyDon'tAsK TheStupidOnesBelum ada peringkat
- Community Health Nursing Review (Edited)Dokumen407 halamanCommunity Health Nursing Review (Edited)api-2658787991% (35)
- Specific Heat ProblemsDokumen4 halamanSpecific Heat ProblemskhenBelum ada peringkat
- Community Health Nursing: I - Definition of TermsDokumen25 halamanCommunity Health Nursing: I - Definition of TermsRichard Ines Valino97% (29)
- IntrodutionDokumen21 halamanIntrodutionDon'tAsK TheStupidOnesBelum ada peringkat
- Nursing Review BulletsDokumen125 halamanNursing Review BulletsROBERT C. REÑA, BSN, RN, MAN (ue)96% (46)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- TFN - BennerDokumen1 halamanTFN - BennerNikkaDablioBelum ada peringkat
- Commercial Dispatch Eedition 6-6-19Dokumen12 halamanCommercial Dispatch Eedition 6-6-19The DispatchBelum ada peringkat
- Broken Ankle: The Story of The Break & RecoveryDokumen6 halamanBroken Ankle: The Story of The Break & RecoveryJane GilgunBelum ada peringkat
- DhakaDokumen427 halamanDhakaArafat Hussain83% (6)
- CONTOH ETHICAL CONSIDERATION Kuliah S2Dokumen7 halamanCONTOH ETHICAL CONSIDERATION Kuliah S2Filia SofiaBelum ada peringkat
- My Modern-Day Hero: SourceDokumen2 halamanMy Modern-Day Hero: SourceDennis RosayagaBelum ada peringkat
- Guideline on Management of Hyperemesis GravidarumDokumen12 halamanGuideline on Management of Hyperemesis GravidarumSiska FriedmanBelum ada peringkat
- GOSH E-Health Project Launch Brochure and Screen GrabsDokumen14 halamanGOSH E-Health Project Launch Brochure and Screen GrabsDavid South100% (1)
- Tugas Ebp FixDokumen18 halamanTugas Ebp FiximranBelum ada peringkat
- Case Study, Chapter 3, Critical Thinking, Ethical Decision Making, and The Nursing ProcessDokumen2 halamanCase Study, Chapter 3, Critical Thinking, Ethical Decision Making, and The Nursing Processclyde i am0% (1)
- Emergency Contac Number and Flow ChardDokumen1 halamanEmergency Contac Number and Flow Charddedy ombehBelum ada peringkat
- Nurses Leading Primary Health Care: Delivering Quality, Serving CommunitiesDokumen39 halamanNurses Leading Primary Health Care: Delivering Quality, Serving Communitiesnecropsi100% (1)
- Dialogue of Heart Failure Patients Accompanied by A Child With A NurseDokumen2 halamanDialogue of Heart Failure Patients Accompanied by A Child With A NurseWilda NingsihBelum ada peringkat
- Golf Journal 2011Dokumen78 halamanGolf Journal 2011duanereadeBelum ada peringkat
- #1. "Princess/Prince/Diva": Slang and Code WordsDokumen5 halaman#1. "Princess/Prince/Diva": Slang and Code WordsAngie MandeoyaBelum ada peringkat
- 1 Guidelines For Anesthetic Management in Clinical PracticeDokumen54 halaman1 Guidelines For Anesthetic Management in Clinical PracticeAMVAC RomaniaBelum ada peringkat
- Akshitha Sreerangapuri - Interview Assessment 1 - Submit - MajorDokumen2 halamanAkshitha Sreerangapuri - Interview Assessment 1 - Submit - Majorapi-324384458Belum ada peringkat
- About The AuthorDokumen1 halamanAbout The AuthorErsya MusLih AnshoriBelum ada peringkat
- Screenplay ST VincentDokumen112 halamanScreenplay ST VincentJeyandan NadarajahBelum ada peringkat
- CPT Manual-Appendix A - 10.6.2013 10-04-52 PMDokumen6 halamanCPT Manual-Appendix A - 10.6.2013 10-04-52 PMEmmanuel FrutosBelum ada peringkat
- Varanasi City ProfileDokumen4 halamanVaranasi City ProfileJohn Nunez100% (1)
- Forgery SC Parmanand PatelDokumen12 halamanForgery SC Parmanand PateladvopaulBelum ada peringkat
- Short Film Analysis: UnwindDokumen4 halamanShort Film Analysis: UnwindWilhelminaDennessBelum ada peringkat
- 2011 Article 162 PDFDokumen8 halaman2011 Article 162 PDFJ.J.Belum ada peringkat
- RCC CaseDokumen1 halamanRCC CaseAnurag GahlawatBelum ada peringkat
- Sample Article in Outpatient DepartmentDokumen2 halamanSample Article in Outpatient DepartmentRodney Beltran SubaranBelum ada peringkat
- 1466 5426 3 PBDokumen3 halaman1466 5426 3 PBSanchithya AriyawanshaBelum ada peringkat
- Project of Shree Shivanand Mission Trust Hospital RajkotDokumen22 halamanProject of Shree Shivanand Mission Trust Hospital RajkotDevvrat SukhwalBelum ada peringkat
- Privilege Speech - Kiwanis January 20Dokumen3 halamanPrivilege Speech - Kiwanis January 20bubblingbrookBelum ada peringkat
- Proposal MedicalDokumen3 halamanProposal MedicalPraneeta Krishna DesaiBelum ada peringkat