Anda mungkin juga menyukai
- 2017 Article 2147 PDFDokumen6 halaman2017 Article 2147 PDFanon_235643778Belum ada peringkat
- Epidemiology of Plasmodium Infections in Flores Island, Indonesia Using Real-Time PCRDokumen9 halamanEpidemiology of Plasmodium Infections in Flores Island, Indonesia Using Real-Time PCRTeuku M Arief YaminBelum ada peringkat
- 4550-Article Text-8533-1-10-20200625Dokumen6 halaman4550-Article Text-8533-1-10-20200625joy sambuagaBelum ada peringkat
- Two Clusters of Plasmodium Knowlesi Cases in A Malaria Elimination Area, Sabang Municipality, Aceh, IndonesiaDokumen10 halamanTwo Clusters of Plasmodium Knowlesi Cases in A Malaria Elimination Area, Sabang Municipality, Aceh, IndonesiaEdza Aria Wikurendra, S.KL, M.KLBelum ada peringkat
- 2995 2495 1 PBDokumen10 halaman2995 2495 1 PBRen'z RezpectorBelum ada peringkat
- JournalDokumen12 halamanJournalDio SukardiBelum ada peringkat
- Kondisi Lingkungan Pemukiman Yang Tidak Sehat Berisiko Terhadap Kejadian Leptospirosis (Studi Kasus Di Kota Semarang)Dokumen9 halamanKondisi Lingkungan Pemukiman Yang Tidak Sehat Berisiko Terhadap Kejadian Leptospirosis (Studi Kasus Di Kota Semarang)Dedi MulyadiBelum ada peringkat
- Mobile Phones Improve Case Detection and Management of Malaria in Rural BangladeshDokumen8 halamanMobile Phones Improve Case Detection and Management of Malaria in Rural BangladeshTamburaka Maulana Da'iBelum ada peringkat
- s12936 017 2110 7Dokumen12 halamans12936 017 2110 7M Franck MakongaBelum ada peringkat
- Adriana Et AlDokumen9 halamanAdriana Et AlSuhana KhanBelum ada peringkat
- Jurnal Gis FilariasisDokumen13 halamanJurnal Gis FilariasisYoga KristhianBelum ada peringkat
- Ifat 2 MalariaDokumen6 halamanIfat 2 MalariaIFan Erian KurniawanBelum ada peringkat
- Durgarani A (53-56)Dokumen5 halamanDurgarani A (53-56)Anonymous RxWzgOBelum ada peringkat
- Sensitivity of Rapid Diagnostic Test and Microscopy in Malaria Diagnosis in Iva-Valley Suburb, EnuguDokumen4 halamanSensitivity of Rapid Diagnostic Test and Microscopy in Malaria Diagnosis in Iva-Valley Suburb, EnuguSMA N 1 TOROHBelum ada peringkat
- Some Info About DengueDokumen15 halamanSome Info About DenguejonyBelum ada peringkat
- Elga Yunus - Journal - Stikes Nas (English)Dokumen11 halamanElga Yunus - Journal - Stikes Nas (English)ELGA YUNUSBelum ada peringkat
- Knowlesi, P. Falciparum, and P. VivaxDokumen8 halamanKnowlesi, P. Falciparum, and P. VivaxW GiBsonBelum ada peringkat
- Multidrug Resistant Tuberculosis Outbreak in South 7Dokumen2 halamanMultidrug Resistant Tuberculosis Outbreak in South 7Simbakutty VenkataramananBelum ada peringkat
- 529 With Cover Page v2Dokumen8 halaman529 With Cover Page v2Dwita Ayu IsrawatiBelum ada peringkat
- Andriamandimby S, 2013 PDFDokumen6 halamanAndriamandimby S, 2013 PDFmangiemrBelum ada peringkat
- 28151-Article Text-90383-1-10-20191231 PDFDokumen7 halaman28151-Article Text-90383-1-10-20191231 PDFDevi Hindira AlfaridaBelum ada peringkat
- Jurnal 2Dokumen16 halamanJurnal 2grace liwantoBelum ada peringkat
- Garuda 1424082Dokumen11 halamanGaruda 1424082Evi sopiahBelum ada peringkat
- Analisis Pola Persebaran Penyakit Leptospirosis Di Kota Semarang Tahun 2014 - 2016Dokumen11 halamanAnalisis Pola Persebaran Penyakit Leptospirosis Di Kota Semarang Tahun 2014 - 2016Evi sopiahBelum ada peringkat
- Trends of Human Plague, Madagascar, 1998-2016Dokumen9 halamanTrends of Human Plague, Madagascar, 1998-2016Pawan MishraBelum ada peringkat
- A Study of Thrombocytopenia in Malaria and Its Prognostic SignificanceDokumen6 halamanA Study of Thrombocytopenia in Malaria and Its Prognostic SignificanceBobby Faisyal RakhmanBelum ada peringkat
- Clinical and Hemoglobin Profile of Malaria Patients in Karitas Hospital, Southwest Sumba District, Indonesia DURING 2017Dokumen8 halamanClinical and Hemoglobin Profile of Malaria Patients in Karitas Hospital, Southwest Sumba District, Indonesia DURING 2017puskesmasBelum ada peringkat
- Jurnal Malaria Deteksi DiniDokumen6 halamanJurnal Malaria Deteksi DiniAhmad SyawqiBelum ada peringkat
- Research Article Plasmodium FalciparumDokumen5 halamanResearch Article Plasmodium FalciparumIsmail IkhsanBelum ada peringkat
- Fajriyah 2017 IOP Conf. Ser. Earth Environ. Sci. 55 012013Dokumen11 halamanFajriyah 2017 IOP Conf. Ser. Earth Environ. Sci. 55 012013Insyirah DaudBelum ada peringkat
- Sani Ashiru ProjectDokumen13 halamanSani Ashiru Projectassunny.abdulBelum ada peringkat
- Draft Research ProposalDokumen5 halamanDraft Research ProposalNursakmawani Abdul RafarBelum ada peringkat
- Reservoir and Distribution Case Studies Leptospirosis in Gresik Regency in 2010Dokumen12 halamanReservoir and Distribution Case Studies Leptospirosis in Gresik Regency in 2010alfihuseinBelum ada peringkat
- Necator Americanus & Ancylostoma DuodenaleDokumen12 halamanNecator Americanus & Ancylostoma DuodenaleSalsabila Putri AmrilBelum ada peringkat
- 8 Malaria Is An Uncommon Cause of Adult Sepsis in SouthDokumen9 halaman8 Malaria Is An Uncommon Cause of Adult Sepsis in SouthAhmad Zaki YamaniBelum ada peringkat
- MALÁRIA No Celldyn TrabalhoDokumen5 halamanMALÁRIA No Celldyn TrabalhoAlexandre MedeirosBelum ada peringkat
- 35 Iajps35052018-1 PDFDokumen4 halaman35 Iajps35052018-1 PDFiajpsBelum ada peringkat
- IMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSDokumen4 halamanIMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSjavelezhBelum ada peringkat
- Out 65Dokumen8 halamanOut 65Diandhara NuryadinBelum ada peringkat
- Megbaru 10 PDFDokumen7 halamanMegbaru 10 PDFMegbaruBelum ada peringkat
- Typhoid Review pntd.0004785 PDFDokumen16 halamanTyphoid Review pntd.0004785 PDFKhotibul maulanaBelum ada peringkat
- Binax 28Dokumen4 halamanBinax 28pieterinpretoria391Belum ada peringkat
- Trend and Spatial Pattern Analysis of Dengue Cases in Northeast MsiaDokumen8 halamanTrend and Spatial Pattern Analysis of Dengue Cases in Northeast Msiaqusyairi_muhammadBelum ada peringkat
- تنزيلDokumen8 halamanتنزيلSuraBelum ada peringkat
- Gambaran RDT MalariaDokumen6 halamanGambaran RDT Malariarasmanto okeBelum ada peringkat
- Rapid Diagnostic Tests Failing To Detect Investigation of Reported False Negative RDT ResultsDokumen6 halamanRapid Diagnostic Tests Failing To Detect Investigation of Reported False Negative RDT ResultsMissing ManBelum ada peringkat
- Riginal Tudy: Sexually Transmitted Diseases Volume 43, Number 10, October 2016Dokumen9 halamanRiginal Tudy: Sexually Transmitted Diseases Volume 43, Number 10, October 2016Andhika DBelum ada peringkat
- Cancer ImmunologyDokumen8 halamanCancer ImmunologyMss RavianBelum ada peringkat
- A Studey On The Epidemiological Characteristics and Infectious Forecast Model of Malaria at Guangzhou Airport Among Chinese Returnees From AfricaDokumen7 halamanA Studey On The Epidemiological Characteristics and Infectious Forecast Model of Malaria at Guangzhou Airport Among Chinese Returnees From AfricaShahir SharifiBelum ada peringkat
- Journal Feng LiaoDokumen19 halamanJournal Feng LiaoDewi KUBelum ada peringkat
- Translate Jurnal NopiDokumen14 halamanTranslate Jurnal NopiMaldi PrasetyoBelum ada peringkat
- Trombosit Dan ParasitDokumen5 halamanTrombosit Dan ParasitSaraswati Wulandari HartonoBelum ada peringkat
- Jurnal Keperawatan MuhammadiyahDokumen10 halamanJurnal Keperawatan MuhammadiyahSeptine Eka PutriBelum ada peringkat
- Post-Renal Transplant Infections: Single-Center Experience From NigeriaDokumen9 halamanPost-Renal Transplant Infections: Single-Center Experience From NigeriaRaquel JimenezBelum ada peringkat
- Research Article Aedes Vector Indices and ClimaticDokumen12 halamanResearch Article Aedes Vector Indices and ClimaticRidwan gorontaloBelum ada peringkat
- Malaria in The 21st Century - Still A Threatening Problem: Predrag Čanović, Biljana Popovska-Jovičić, Milorad PavlovićDokumen4 halamanMalaria in The 21st Century - Still A Threatening Problem: Predrag Čanović, Biljana Popovska-Jovičić, Milorad Pavlovićbiljanapopovskaj79Belum ada peringkat
- Inayat Ullah Et Al 2019 PDFDokumen4 halamanInayat Ullah Et Al 2019 PDFMehwish NawazBelum ada peringkat
- ID Analisis Spasial Pengaruh Faktor LingkunDokumen10 halamanID Analisis Spasial Pengaruh Faktor Lingkunlele ikanBelum ada peringkat
- Utility of qSOFA and Modified SOFA in Severe Malaria Presenting As SepsisDokumen13 halamanUtility of qSOFA and Modified SOFA in Severe Malaria Presenting As SepsisAhmad Zaki YamaniBelum ada peringkat
- Diagnostic Imaging of Novel Coronavirus PneumoniaDari EverandDiagnostic Imaging of Novel Coronavirus PneumoniaMinming ZhangBelum ada peringkat
- Question Report 2478Dokumen11 halamanQuestion Report 2478Raghav gupta100% (1)
- Animal Bite FormDokumen1 halamanAnimal Bite FormReignmar MontañoBelum ada peringkat
- Exporters DirectoryDokumen1 halamanExporters DirectoryMipta KurniawanBelum ada peringkat
- Shed No Tears For The Defeated by William Hunt-VincentDokumen30 halamanShed No Tears For The Defeated by William Hunt-VincentAustin Macauley Publishers Ltd.Belum ada peringkat
- XtendaDokumen2 halamanXtendaAlexis CoronadoBelum ada peringkat
- Chicken Wing DissectionDokumen13 halamanChicken Wing DissectionJaga_Sahsiny_1Belum ada peringkat
- Kamasutra LengkapDokumen104 halamanKamasutra LengkapTjap TjoeanBelum ada peringkat
- Cell As The Basic Unit of LifeDokumen48 halamanCell As The Basic Unit of Lifeharshana rajagopalBelum ada peringkat
- Taban Lo Liyong Fixions and Other StoriesDokumen27 halamanTaban Lo Liyong Fixions and Other StoriesStacy Hardy100% (1)
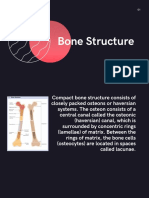
- Topic PPT Bone StructureDokumen14 halamanTopic PPT Bone StructureMoonBelum ada peringkat
- Yh 5302Dokumen17 halamanYh 5302Elizabeth FernandezBelum ada peringkat
- Small Pox Is DeadDokumen46 halamanSmall Pox Is Deadtummalapalli venkateswara raoBelum ada peringkat
- Lethal Dose 50Dokumen18 halamanLethal Dose 50h3cn1r3Belum ada peringkat
- Microsoft Word - The BloodDokumen16 halamanMicrosoft Word - The BloodMelanie Fleckner0% (3)
- MMRDokumen84 halamanMMRKelly YeowBelum ada peringkat
- Maxillary Superimposition - A Comparison of Three Methods For Cephalometric Evaluation of Growth and Treatment ChangeDokumen10 halamanMaxillary Superimposition - A Comparison of Three Methods For Cephalometric Evaluation of Growth and Treatment ChangeNataly ComettaBelum ada peringkat
- Homoeopathic Rmedy For ShockDokumen2 halamanHomoeopathic Rmedy For ShockSuhas IngaleBelum ada peringkat
- Exam (1) On Unit (1) :: Connect Plus 4 - 1st TermDokumen12 halamanExam (1) On Unit (1) :: Connect Plus 4 - 1st TermHassan k1455 rashidBelum ada peringkat
- MasterMind 2 Unit 1 WordlistDokumen3 halamanMasterMind 2 Unit 1 WordlistRolando Guzman MartinezBelum ada peringkat
- Class 3 EVS Question Bank 1Dokumen8 halamanClass 3 EVS Question Bank 1ᴅᴇᴇᴘ ᴘʀᴀᴋᴀsʜ ᴍᴏᴅɪ xɪ-ᴅBelum ada peringkat
- Easy Kitten With Heart Amigurumi PDF Free PatternDokumen6 halamanEasy Kitten With Heart Amigurumi PDF Free PatternSandra100% (1)
- Diagnostic Traditional MedicineDokumen225 halamanDiagnostic Traditional MedicineJRA100% (17)
- Dragonix - DM Options, Monster Talents IIDokumen246 halamanDragonix - DM Options, Monster Talents IIJolticsy Rules100% (8)
- (tailieudieuky.com) Fanpage TÀI LIỆU TIẾNG ANH NÂNG CAO KỲ THI THỬ CHỌN HỌC SINH GIỎI QUỐC GIA THPT năm 2022 có đáp ánDokumen22 halaman(tailieudieuky.com) Fanpage TÀI LIỆU TIẾNG ANH NÂNG CAO KỲ THI THỬ CHỌN HỌC SINH GIỎI QUỐC GIA THPT năm 2022 có đáp ánHuỳnh Ngan AnhBelum ada peringkat
- The Good Dinosaur ReviewDokumen3 halamanThe Good Dinosaur ReviewAbdul Rashid Abdul RahmanBelum ada peringkat
- Test Dos InglesDokumen4 halamanTest Dos Inglesgbøniillaa75% (4)
- Material Safety Data Sheet: Hitec 6473 Gasoline Fuel AdditiveDokumen7 halamanMaterial Safety Data Sheet: Hitec 6473 Gasoline Fuel Additiveamiller1987Belum ada peringkat
- Food and Man 1Dokumen25 halamanFood and Man 1Rejoice Gumboc MabilogBelum ada peringkat
- Y 0870 e 51Dokumen12 halamanY 0870 e 51Yohanes BaptistaBelum ada peringkat
- Laktosa Mempertahankan Daya Hidup Spermatozoa Kambing Peranakan Etawah Yang Dipreservasi Dengan Plasma Semen Domba PrianganDokumen8 halamanLaktosa Mempertahankan Daya Hidup Spermatozoa Kambing Peranakan Etawah Yang Dipreservasi Dengan Plasma Semen Domba Prianganachmad setiyonoBelum ada peringkat