Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
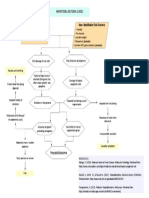
- Hospital Use CaseDokumen3 halamanHospital Use Caseprashant gauravBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- VDL Biopsy SubmissionDokumen26 halamanVDL Biopsy SubmissionThomas Karl Anthony QUILANGBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Recent Advances in Diagnosis, Treatment and Prevention of Hepatocellular Carcinoma (HCC)Dokumen65 halamanRecent Advances in Diagnosis, Treatment and Prevention of Hepatocellular Carcinoma (HCC)amal.fathullahBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Questions:: Exercise 4. Bioethical Dilemma of Gene TherapyDokumen2 halamanQuestions:: Exercise 4. Bioethical Dilemma of Gene Therapyrjay manaloBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- ADULT Nutrition Screening Questionnaire 2Dokumen1 halamanADULT Nutrition Screening Questionnaire 2Alejandra López SalasBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Non-Modifiable Risk Factors: Hepatoblastoma CaseDokumen1 halamanNon-Modifiable Risk Factors: Hepatoblastoma CaseALYSSA AGATHA FELIZARDOBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Transverse MyelitisDokumen7 halamanTransverse MyelitisAmr BashaBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- PNSS Drug StudyDokumen2 halamanPNSS Drug Studyrain peregrinoBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Cadila Pharmaceuticals Ltd. ProfileDokumen3 halamanCadila Pharmaceuticals Ltd. Profilemail_garaiBelum ada peringkat
- Jurnal Porio 1Dokumen3 halamanJurnal Porio 1Neo YustindraBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Intrauterine Fetal DeathDokumen6 halamanIntrauterine Fetal DeathKezia Marsilina100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- BASIC PerimetryDokumen28 halamanBASIC PerimetryDwi Atikah SariBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Gra ViolaDokumen8 halamanGra ViolaAnthony SullivanBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- X Ray ProtocolDokumen2 halamanX Ray ProtocolKhaidir AlimBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- KodingDokumen12 halamanKodingAva Vav100% (1)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- 88 FinalDokumen4 halaman88 FinalEshiebel OrganistaBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Focal Fibrous Hyperplasia: A Clinical and Histological InsightDokumen3 halamanFocal Fibrous Hyperplasia: A Clinical and Histological InsightIJAR JOURNALBelum ada peringkat
- Second Medical Use CountriesDokumen5 halamanSecond Medical Use CountriesAnonymous AWcEiTj5u0Belum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Annotated BibliographyDokumen5 halamanAnnotated Bibliographyapi-286443025Belum ada peringkat
- Ake Quick Action If Someone Is Choking On A Swallowed ObjectDokumen29 halamanAke Quick Action If Someone Is Choking On A Swallowed ObjectYAMINIPRIYANBelum ada peringkat
- Frequency DR Hulda Clark ZapperDokumen45 halamanFrequency DR Hulda Clark ZapperkwbutterfliesBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Nadira Duwi 3191028 Naufal HafidDokumen61 halamanNadira Duwi 3191028 Naufal HafidNadira RaraBelum ada peringkat
- Immunology: 'S CompanionsDokumen74 halamanImmunology: 'S CompanionsRoahit RajanBelum ada peringkat
- Post Graduate Diploma in Clinical Cardiology (PGDCC) : Mcc-004: Common Cardio-Vascular Diseases - IiDokumen8 halamanPost Graduate Diploma in Clinical Cardiology (PGDCC) : Mcc-004: Common Cardio-Vascular Diseases - IiBoda JyothiBelum ada peringkat
- PolytraumaDokumen41 halamanPolytraumaFrederick Mars UntalanBelum ada peringkat
- Ananth Narayan and Paniker 11th EditionDokumen42 halamanAnanth Narayan and Paniker 11th EditionArjun Kandara50% (2)
- The Impact of Menstrual Periods On Performance of Female WorkersDokumen5 halamanThe Impact of Menstrual Periods On Performance of Female WorkersEiman Khowaja (22GJKB-CLSTEC)Belum ada peringkat
- Breast Cancer ScreeningDokumen7 halamanBreast Cancer ScreeninglucaassuntiBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- 4th Year Write Up 2 - Int. MedDokumen11 halaman4th Year Write Up 2 - Int. MedLoges TobyBelum ada peringkat
- Golongan ObatDokumen29 halamanGolongan ObatMala PanoBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)