Anda mungkin juga menyukai
- Prehospital Practice: hypothetically speaking: From classroom to paramedic practice Volume 1 Second editionDari EverandPrehospital Practice: hypothetically speaking: From classroom to paramedic practice Volume 1 Second editionBelum ada peringkat
- 4 Pre-Eclampsia & Eclampsia - Eclampsia - Scenario 1Dokumen4 halaman4 Pre-Eclampsia & Eclampsia - Eclampsia - Scenario 1rhtyehBelum ada peringkat
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesDari EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesPenilaian: 5 dari 5 bintang5/5 (2)
- 5 PPH - Scenario 1Dokumen4 halaman5 PPH - Scenario 1mjgmhgfvBelum ada peringkat
- The Basics: A Comprehensive Outline of Nursing School ContentDari EverandThe Basics: A Comprehensive Outline of Nursing School ContentPenilaian: 5 dari 5 bintang5/5 (3)
- 3 SEPSIS - Puerperal Sepsis - Scenario 1Dokumen4 halaman3 SEPSIS - Puerperal Sepsis - Scenario 1iokujyhngrvfedBelum ada peringkat
- 3 SEPSIS - Septic Miscarriage - Scenario 2Dokumen4 halaman3 SEPSIS - Septic Miscarriage - Scenario 2iokujyhngrvfedBelum ada peringkat
- DR Manual 2022Dokumen17 halamanDR Manual 2022Vaniegrace Angel BalagonBelum ada peringkat
- ESMOE-EOST: Birth at HomeDokumen4 halamanESMOE-EOST: Birth at HomeSlindy Noty MtetwaBelum ada peringkat
- Unit VI L&D Case StudyDokumen6 halamanUnit VI L&D Case StudyBrooke Misty Ann BaileyBelum ada peringkat
- Case Study 111Dokumen4 halamanCase Study 111jhan jhanBelum ada peringkat
- Bemonc - S-Cort - Osce 1, 2 and 3Dokumen6 halamanBemonc - S-Cort - Osce 1, 2 and 3TayeBelum ada peringkat
- Nonstress Test (NST) : It Is A Test That Assess The Fetal Heart Rate in Correspondence To Fetal Movements at To AssessDokumen4 halamanNonstress Test (NST) : It Is A Test That Assess The Fetal Heart Rate in Correspondence To Fetal Movements at To AssessAnuradha MauryaBelum ada peringkat
- Management of Woman During First Stage of Labour Management of Woman During First Stage of LabourDokumen21 halamanManagement of Woman During First Stage of Labour Management of Woman During First Stage of LabourKinjal Vasava67% (3)
- Case Simulation 115Dokumen6 halamanCase Simulation 115Cheska PalomaBelum ada peringkat
- Pediatric Nursing Resource UnitDokumen36 halamanPediatric Nursing Resource UnitDaryl Adrian RecaidoBelum ada peringkat
- Case Study 115Dokumen6 halamanCase Study 115Jonah MaasinBelum ada peringkat
- Labor and DeliveryDokumen74 halamanLabor and DeliveryRussel Kate SulangBelum ada peringkat
- Case Simu 115Dokumen5 halamanCase Simu 115Princess Levie CenizaBelum ada peringkat
- Cara BertaniDokumen9 halamanCara BertaniDodi MulyadiBelum ada peringkat
- NCM 107 RLE Topic 5 Nov 9-13, 2020Dokumen13 halamanNCM 107 RLE Topic 5 Nov 9-13, 2020mirai desu100% (2)
- Leopold's Maneuver Retdem ScriptDokumen4 halamanLeopold's Maneuver Retdem ScriptariadnebabasaBelum ada peringkat
- Labor WatchDokumen35 halamanLabor WatchLawrence Steve Beronio MapaBelum ada peringkat
- MCN Rle Instruments and Setting Up of DR TableDokumen4 halamanMCN Rle Instruments and Setting Up of DR TableJay EstrellaBelum ada peringkat
- DR Technique Checklist101Dokumen8 halamanDR Technique Checklist101Christine Joy MolinaBelum ada peringkat
- DR Technique ChecklistDokumen8 halamanDR Technique ChecklistChristine Joy MolinaBelum ada peringkat
- Intrapartum: Delivery Room Technique PurposeDokumen8 halamanIntrapartum: Delivery Room Technique PurposeRoshin TejeroBelum ada peringkat
- Intrapartum: Delivery Room Technique PurposeDokumen8 halamanIntrapartum: Delivery Room Technique PurposeChristine Joy MolinaBelum ada peringkat
- Nursing Management During Stages of Labor and Delivery UpdatedDokumen40 halamanNursing Management During Stages of Labor and Delivery UpdatedCharlmagne LinnamBelum ada peringkat
- Managament of The 2nd Stage of LabourDokumen59 halamanManagament of The 2nd Stage of LabourJSeasharkBelum ada peringkat
- Obgyn SL1Dokumen39 halamanObgyn SL1mustafe omarBelum ada peringkat
- Suctioning The NewbornDokumen7 halamanSuctioning The Newbornzeren.angeles.ihsBelum ada peringkat
- DR Technique Checklist 1Dokumen10 halamanDR Technique Checklist 1Omar James Abdulgani LimBelum ada peringkat
- Nursing Management of During Stages of Labor and Delivery UpdatedDokumen60 halamanNursing Management of During Stages of Labor and Delivery UpdatedSherlyn Miranda GarcesBelum ada peringkat
- Intrapartum: Delivery Room Technique PurposeDokumen7 halamanIntrapartum: Delivery Room Technique Purposesharmena harunBelum ada peringkat
- DR Technique ChecklistDokumen8 halamanDR Technique ChecklistPATRICIA JULIANNE CASTAÑETO RIVERABelum ada peringkat
- NFDN 2004 - Unit 4.3 - JLB StudentDokumen43 halamanNFDN 2004 - Unit 4.3 - JLB StudentkendrabooboooBelum ada peringkat
- Physiology of 1st Stage of LaborDokumen134 halamanPhysiology of 1st Stage of LaborVijith.V.kumar50% (2)
- Cme NRPDokumen73 halamanCme NRPpayapaya.pipacyclineBelum ada peringkat
- NPR FinalDokumen13 halamanNPR FinalMohamed ElkadyBelum ada peringkat
- EINC Handout by Nicole Honrado BSN 2ADokumen7 halamanEINC Handout by Nicole Honrado BSN 2A2A - Nicole Marrie HonradoBelum ada peringkat
- Management of First Stage of Labour: Prepared By: Nirsuba Gurung Assistant Lecturer MsonDokumen55 halamanManagement of First Stage of Labour: Prepared By: Nirsuba Gurung Assistant Lecturer MsonBharat ThapaBelum ada peringkat
- Ceklis APN 1920Dokumen12 halamanCeklis APN 1920wahyu kijang ramadhanBelum ada peringkat
- Intrapartal Period: Methods of Pain ManagementDokumen7 halamanIntrapartal Period: Methods of Pain Managementdarkscaler100% (2)
- Be MOCDokumen24 halamanBe MOCshobekai30Belum ada peringkat
- Management of First Stage of LabourDokumen55 halamanManagement of First Stage of LabourBharat ThapaBelum ada peringkat
- 15 EmOC Labour & P'gram 2016 FINALDokumen45 halaman15 EmOC Labour & P'gram 2016 FINALDavina DakapBelum ada peringkat
- NCM107 MCN - Pedia Nursing SL Semifinal HandoutsDokumen17 halamanNCM107 MCN - Pedia Nursing SL Semifinal HandoutsLillabinBelum ada peringkat
- Osce Checklist 01: em Ergency Tri Age O F New Born: # Steps Score ParticipantsDokumen41 halamanOsce Checklist 01: em Ergency Tri Age O F New Born: # Steps Score ParticipantsVandanaBelum ada peringkat
- Intrapartum DR TechniqueDokumen10 halamanIntrapartum DR TechniqueAl-waleed JulkanainBelum ada peringkat
- Intrapartum DR TechniqueDokumen10 halamanIntrapartum DR TechniqueAl-waleed JulkanainBelum ada peringkat
- Normal Spontaneous Vaginal Delivery: IndicationsDokumen7 halamanNormal Spontaneous Vaginal Delivery: IndicationsT helper CellsBelum ada peringkat
- Cardiopulmonary Resuscitation For Adults Pedia and InfantsDokumen35 halamanCardiopulmonary Resuscitation For Adults Pedia and InfantsAnna Carmela Pillora MelendezBelum ada peringkat
- Airway Management For InternsDokumen2 halamanAirway Management For InternsZllison Mae Teodoro MangabatBelum ada peringkat
- 9 Labor and DeliveryDokumen6 halaman9 Labor and DeliveryUri Perez MontedeRamosBelum ada peringkat
- BCS General Principles of Physical ExaminationDokumen43 halamanBCS General Principles of Physical ExaminationPande Indra PremanaBelum ada peringkat
- Stage 1Dokumen10 halamanStage 1JosephNawenBelum ada peringkat
- Or - Plan of ActivitiesDokumen1 halamanOr - Plan of ActivitiesJessa AdenigBelum ada peringkat
- RPS 14Dokumen19 halamanRPS 14Ridanna HartateanaBelum ada peringkat
- Bemonc Section 5-1Dokumen24 halamanBemonc Section 5-1JUANJOSEFOXBelum ada peringkat
- Prof. Vijaya Lakshmi Nag CVDokumen24 halamanProf. Vijaya Lakshmi Nag CVanislinek15Belum ada peringkat
- Fundamentals of Nursing Part 5Dokumen36 halamanFundamentals of Nursing Part 5Honeylie Patricio100% (1)
- Planned Parenthood and Students Knowledge of Contraceptive MethodsDokumen10 halamanPlanned Parenthood and Students Knowledge of Contraceptive MethodssncuBelum ada peringkat
- Handbook of Institutional Pharmacy Practice Chapter 2Dokumen14 halamanHandbook of Institutional Pharmacy Practice Chapter 2Joe FX TraderBelum ada peringkat
- Bag TechniqueDokumen4 halamanBag TechniqueCharlie Cotoner FalgueraBelum ada peringkat
- Aspirating Drugs From Ampules and VialsDokumen9 halamanAspirating Drugs From Ampules and VialsmariallenBelum ada peringkat
- PE and HEALTH 9 PA-1Dokumen3 halamanPE and HEALTH 9 PA-1Alma Bernadette RuivivarBelum ada peringkat
- Intersono IVF ClinicDokumen21 halamanIntersono IVF ClinicINTERSONOBelum ada peringkat
- SDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionDokumen5 halamanSDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionYwagar YwagarBelum ada peringkat
- NEWBORN CAREPLAN - VEST - FISTULA SurgicalDokumen16 halamanNEWBORN CAREPLAN - VEST - FISTULA SurgicalArchana SahuBelum ada peringkat
- HBP 2.0-For Website V2 PDFDokumen26 halamanHBP 2.0-For Website V2 PDFapurva shahBelum ada peringkat
- Migraine Diaries PDFDokumen4 halamanMigraine Diaries PDFDr.Gopinath SaravananBelum ada peringkat
- PT. PLI - ID CardDokumen1 halamanPT. PLI - ID CardAlam DooBelum ada peringkat
- Incisionvsexcisionvsresection 140319203037 Phpapp02Dokumen8 halamanIncisionvsexcisionvsresection 140319203037 Phpapp02noto susanto100% (1)
- MS GuldaneDokumen22 halamanMS GuldaneKhyy SafitryBelum ada peringkat
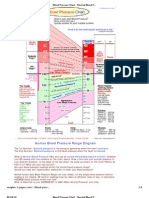
- Blood Pressure ChartDokumen4 halamanBlood Pressure ChartPixelateBelum ada peringkat
- Disseminated Intravascular Coagulation Initial Score As A Predictor ofDokumen6 halamanDisseminated Intravascular Coagulation Initial Score As A Predictor ofPriska ForceveeanaBelum ada peringkat
- Personal Accident BrochureDokumen2 halamanPersonal Accident BrochureAmar DixitBelum ada peringkat
- Hypertension and Herbal Plant For Its Treatment: A ReviewDokumen1 halamanHypertension and Herbal Plant For Its Treatment: A Reviewdyan ayu puspariniBelum ada peringkat
- Clinico Histological Evaluation of Dentino-Pulpal Complex of DirectDokumen6 halamanClinico Histological Evaluation of Dentino-Pulpal Complex of DirectAle ZuzaBelum ada peringkat
- Treating Musculo-Skeletal Pain With Traditional Chinese MedicineDokumen2 halamanTreating Musculo-Skeletal Pain With Traditional Chinese MedicineocoxodoBelum ada peringkat
- Caronan NDP POLO HKGDokumen23 halamanCaronan NDP POLO HKGKatrine Danielle GuardiansBelum ada peringkat
- Tonsil Cancer: Cedars-Sinai ResourceDokumen4 halamanTonsil Cancer: Cedars-Sinai ResourceSiRa DiktaraBelum ada peringkat
- Gap Report Astha HospitalDokumen49 halamanGap Report Astha HospitalNidhi VijanBelum ada peringkat
- Typhoid Fever: PathophysiologyDokumen10 halamanTyphoid Fever: PathophysiologyDominic Stephen VillacostaBelum ada peringkat
- DM Brochure For NCM 106Dokumen12 halamanDM Brochure For NCM 106Kimsha ConcepcionBelum ada peringkat
- 53-99Z - Book Manuscript-136-1-10-20131122Dokumen119 halaman53-99Z - Book Manuscript-136-1-10-20131122dedex_46Belum ada peringkat
- The Journal of Dermatology - 2020 - Mimura - Japanese Clinical Practice Guidelines For Vascular Anomalies 2017Dokumen46 halamanThe Journal of Dermatology - 2020 - Mimura - Japanese Clinical Practice Guidelines For Vascular Anomalies 2017白石 真土320D008Belum ada peringkat
- Causality Assessment PharmacovigilanceDokumen8 halamanCausality Assessment PharmacovigilanceAnonymous Q0wdNI9Belum ada peringkat
- 2021 CPT CodesDokumen8 halaman2021 CPT CodesSundar RamanathanBelum ada peringkat
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDari EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisPenilaian: 3 dari 5 bintang3/5 (2)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeDari EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeBelum ada peringkat
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDari EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimePenilaian: 3.5 dari 5 bintang3.5/5 (13)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenDari EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenPenilaian: 4 dari 5 bintang4/5 (154)
- Natural Hospital Birth: The Best of Both WorldsDari EverandNatural Hospital Birth: The Best of Both WorldsPenilaian: 5 dari 5 bintang5/5 (33)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayDari EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayPenilaian: 4.5 dari 5 bintang4.5/5 (3)
- What to Expect When You’re Expecting (5th Edition)Dari EverandWhat to Expect When You’re Expecting (5th Edition)Penilaian: 5 dari 5 bintang5/5 (1)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondDari EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondPenilaian: 4.5 dari 5 bintang4.5/5 (39)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouDari EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouBelum ada peringkat
- ADHD Women: A Holistic Approach To ADHD ManagementDari EverandADHD Women: A Holistic Approach To ADHD ManagementPenilaian: 5 dari 5 bintang5/5 (4)
- Awakening Fertility: The Essential Art of Preparing for PregnancyDari EverandAwakening Fertility: The Essential Art of Preparing for PregnancyPenilaian: 4.5 dari 5 bintang4.5/5 (36)
- Crones Don't Whine: Concentrated Wisdom for Juicy WomenDari EverandCrones Don't Whine: Concentrated Wisdom for Juicy WomenPenilaian: 2.5 dari 5 bintang2.5/5 (3)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodDari EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodPenilaian: 5 dari 5 bintang5/5 (33)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionDari EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionPenilaian: 4.5 dari 5 bintang4.5/5 (125)
- Pregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!Dari EverandPregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!Penilaian: 5 dari 5 bintang5/5 (1)
- Medical Bondage: Race, Gender, and the Origins of American GynecologyDari EverandMedical Bondage: Race, Gender, and the Origins of American GynecologyPenilaian: 4.5 dari 5 bintang4.5/5 (75)
- Labor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodDari EverandLabor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodPenilaian: 4.5 dari 5 bintang4.5/5 (28)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.Dari EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Penilaian: 4.5 dari 5 bintang4.5/5 (124)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersDari EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersPenilaian: 4.5 dari 5 bintang4.5/5 (71)
- Spirit Baby: Communicate with Your Unborn Baby. Ease Your BirthDari EverandSpirit Baby: Communicate with Your Unborn Baby. Ease Your BirthPenilaian: 5 dari 5 bintang5/5 (1)
- The Menopause Manifesto: Own Your Health With Facts and FeminismDari EverandThe Menopause Manifesto: Own Your Health With Facts and FeminismPenilaian: 4 dari 5 bintang4/5 (18)
- Nurture: A Modern Guide to Pregnancy, Birth, Early Motherhood—and Trusting Yourself and Your BodyDari EverandNurture: A Modern Guide to Pregnancy, Birth, Early Motherhood—and Trusting Yourself and Your BodyPenilaian: 4.5 dari 5 bintang4.5/5 (14)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondDari EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondPenilaian: 4.5 dari 5 bintang4.5/5 (3)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainDari EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainPenilaian: 4 dari 5 bintang4/5 (14)
- Hormone Balance: A Woman's Guide to Restoring Health and VitalityDari EverandHormone Balance: A Woman's Guide to Restoring Health and VitalityPenilaian: 5 dari 5 bintang5/5 (3)
- Period Repair Manual: Natural Treatment for Better Hormones and Better Periods, 2nd editionDari EverandPeriod Repair Manual: Natural Treatment for Better Hormones and Better Periods, 2nd editionPenilaian: 4.5 dari 5 bintang4.5/5 (28)
- Hypnobirthing: Hypnotherapy for Happy, Healthy MindsDari EverandHypnobirthing: Hypnotherapy for Happy, Healthy MindsPenilaian: 5 dari 5 bintang5/5 (8)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionDari EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionPenilaian: 4 dari 5 bintang4/5 (27)
- The Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityDari EverandThe Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityPenilaian: 4.5 dari 5 bintang4.5/5 (12)