Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Sample Questions: American Board of Medical MicrobiologyDokumen8 halamanSample Questions: American Board of Medical Microbiologyelattar.laila1891Belum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Drug Prefixes and SuffixesDokumen12 halamanDrug Prefixes and SuffixesKENNETH GENER JAMES SOMERA0% (1)
- ChromAgar Brochure BDDokumen16 halamanChromAgar Brochure BDapi-3697331100% (1)
- Peramivir Q and A - Updated 11 - 19 - 09 Final CleanDokumen10 halamanPeramivir Q and A - Updated 11 - 19 - 09 Final Cleanbenny christantoBelum ada peringkat
- Mirjam Van Weissenbruch - Neonatal HypoglycaemiaDokumen57 halamanMirjam Van Weissenbruch - Neonatal Hypoglycaemiabenny christantoBelum ada peringkat
- Antianginal 171115034620Dokumen34 halamanAntianginal 171115034620benny christantoBelum ada peringkat
- Kalimat Inggris 2023Dokumen3 halamanKalimat Inggris 2023benny christantoBelum ada peringkat
- The Pocket Guide To Good Health For AdultsDokumen38 halamanThe Pocket Guide To Good Health For Adultsbenny christantoBelum ada peringkat
- Cervical CancerDokumen60 halamanCervical CancerNova Yuli PrasetyoBelum ada peringkat
- Management of Neuropathic Pain in Dialysis Patients: An Effective Approach With GabapentinDokumen3 halamanManagement of Neuropathic Pain in Dialysis Patients: An Effective Approach With Gabapentinbenny christantoBelum ada peringkat
- Drug Adjusting in CKDDokumen10 halamanDrug Adjusting in CKDgigih85Belum ada peringkat
- Iavt03i2p69 PDFDokumen3 halamanIavt03i2p69 PDFBenny Chris TantoBelum ada peringkat
- WHO Recommendations For The Prevention and Treatment of Postpartum HaemorrhageDokumen48 halamanWHO Recommendations For The Prevention and Treatment of Postpartum Haemorrhagebenny christantoBelum ada peringkat
- Fluoroquinolone Benchmarking in Relation To Pharmacokinetic andDokumen5 halamanFluoroquinolone Benchmarking in Relation To Pharmacokinetic andbenny christantoBelum ada peringkat
- Pocket Good ChildDokumen26 halamanPocket Good ChildtheyzBelum ada peringkat
- Cerebrospinal Fluid Shunt Infection A Prospective Study ofDokumen7 halamanCerebrospinal Fluid Shunt Infection A Prospective Study ofbenny christantoBelum ada peringkat
- IDSA Guidelines On The Treatment of MRSA InfectionsDokumen5 halamanIDSA Guidelines On The Treatment of MRSA Infectionsbenny christantoBelum ada peringkat
- WHO Induction LabourDokumen40 halamanWHO Induction LabourshofiyuddinBelum ada peringkat
- WHO Guidelines For Treatment of Cervical Intraepithelial Neoplasia 2-3 and Adenocarcinoma in SituDokumen52 halamanWHO Guidelines For Treatment of Cervical Intraepithelial Neoplasia 2-3 and Adenocarcinoma in Situbenny christantoBelum ada peringkat
- Critical Reviews in Oncology/Hematology: Sandro Barni, Fausto Petrelli, Mary CabidduDokumen10 halamanCritical Reviews in Oncology/Hematology: Sandro Barni, Fausto Petrelli, Mary Cabiddubenny christantoBelum ada peringkat
- Guias Hemorragia PospartoDokumen48 halamanGuias Hemorragia PospartoDai UmqandmcBelum ada peringkat
- Mei Neni - PCVDokumen34 halamanMei Neni - PCVbenny christantoBelum ada peringkat
- Update Management of Asthma Exacerbation - NS - ApprovedDokumen29 halamanUpdate Management of Asthma Exacerbation - NS - Approvedbenny christantoBelum ada peringkat
- ATS GuidelinesDokumen46 halamanATS Guidelinesapi-3847280100% (1)
- 1Dokumen27 halaman1Nada ApriliaBelum ada peringkat
- Pneumonia 1Dokumen12 halamanPneumonia 1Mohammad Izza Naufal FikriBelum ada peringkat
- Mirjam Van Weissenbruch - Neonatal HypoglycaemiaDokumen57 halamanMirjam Van Weissenbruch - Neonatal Hypoglycaemiabenny christantoBelum ada peringkat
- Practice Guidelines For The Managementof Bacterial Meningitis - Idsa.2004Dokumen18 halamanPractice Guidelines For The Managementof Bacterial Meningitis - Idsa.2004Anonymous tMJNIFBelum ada peringkat
- Surviving Sepsis Campaign International.15Dokumen67 halamanSurviving Sepsis Campaign International.15Tanawat SingboonBelum ada peringkat
- SepsisDokumen15 halamanSepsisMedranoReyesLuisinBelum ada peringkat
- EBM Report PDFDokumen4 halamanEBM Report PDFbenny christantoBelum ada peringkat
- Fluoroquinolone Benchmarking in Relation To Pharmacokinetic andDokumen5 halamanFluoroquinolone Benchmarking in Relation To Pharmacokinetic andbenny christantoBelum ada peringkat
- Cerebrospinal Fluid Shunt Infection A Prospective Study ofDokumen7 halamanCerebrospinal Fluid Shunt Infection A Prospective Study ofbenny christantoBelum ada peringkat
- 641-Article Text-1162-1-10-20171110Dokumen19 halaman641-Article Text-1162-1-10-20171110Krishan Kumar sharmaBelum ada peringkat
- Cell Cycle Regulators' Role in Cancer MetabolismDokumen3 halamanCell Cycle Regulators' Role in Cancer MetabolismakyBelum ada peringkat
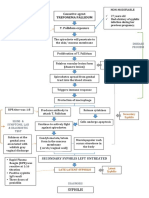
- Pathophysiology of Syphilis ReinfectionDokumen1 halamanPathophysiology of Syphilis Reinfection3S - JOCSON, DENESE NICOLE LEE M.Belum ada peringkat
- Gene Mapping: Biology 20Dokumen5 halamanGene Mapping: Biology 20Soham SenguptaBelum ada peringkat
- Identification of Potentially Pathogenic Bacteria From Tilapia (Oreochromis Niloticus) and Channel Catfish (Clarias Batrachus) Culture in Samarinda, East Kalimantan, IndonesiaDokumen9 halamanIdentification of Potentially Pathogenic Bacteria From Tilapia (Oreochromis Niloticus) and Channel Catfish (Clarias Batrachus) Culture in Samarinda, East Kalimantan, IndonesianurullahfatihBelum ada peringkat
- Genetics Unit Test ReviewDokumen3 halamanGenetics Unit Test ReviewvexelleBelum ada peringkat
- Helminthes IntroDokumen26 halamanHelminthes IntroOrakle mkhwanaziBelum ada peringkat
- Antiviral Drugs Limit Viral Growth Through Multiple MechanismsDokumen90 halamanAntiviral Drugs Limit Viral Growth Through Multiple MechanismsshBelum ada peringkat
- Epithelial-Mesenchymal Crosstalk in Wolffian Duct and FetalDokumen15 halamanEpithelial-Mesenchymal Crosstalk in Wolffian Duct and FetalEletícia SousaBelum ada peringkat
- MK Hemodynamics PathologyDokumen27 halamanMK Hemodynamics PathologyMoses Jr Kazevu100% (1)
- Acid Fast Bacteria: M. Tuberculosis, M. LepraeDokumen22 halamanAcid Fast Bacteria: M. Tuberculosis, M. LepraeelaBelum ada peringkat
- A Few List of VaccinesDokumen23 halamanA Few List of VaccinesPradeepBelum ada peringkat
- HIV NotesDokumen38 halamanHIV NotesMie CorsBelum ada peringkat
- M A D Q: Odel Nswers TO Escriptive UestionsDokumen75 halamanM A D Q: Odel Nswers TO Escriptive UestionsAshritha SirivuriBelum ada peringkat
- Stem Cells and The Skin - Dahl2012Dokumen10 halamanStem Cells and The Skin - Dahl2012ranasoftBelum ada peringkat
- Papaya SipDokumen52 halamanPapaya SipJivin JavaBelum ada peringkat
- Gastroenterology and HepatologyDokumen42 halamanGastroenterology and HepatologyCarlos HernándezBelum ada peringkat
- Chemical Characterization of RNADokumen3 halamanChemical Characterization of RNAAngeloMuñozBelum ada peringkat
- Anatomy of Cornea and Ocular Surface.4Dokumen5 halamanAnatomy of Cornea and Ocular Surface.4Cucută Alexandru-DanielBelum ada peringkat
- Neonatal Intensive Care EyeDokumen2 halamanNeonatal Intensive Care EyewahyuliastingmailcomBelum ada peringkat
- Genetic SL Test: (100 Marks)Dokumen19 halamanGenetic SL Test: (100 Marks)Ritika GulguliaBelum ada peringkat
- Needle Prick InjuryDokumen20 halamanNeedle Prick InjuryThirugnanaThiruBelum ada peringkat
- Interpretation of Peripheral SmearDokumen34 halamanInterpretation of Peripheral Smearswathi bs100% (1)
- Dapi SigmaDokumen2 halamanDapi SigmaeliavvBelum ada peringkat
- Chapter Outline: I Ntrod Uction The Nature of Enzymes LsoenzymesDokumen16 halamanChapter Outline: I Ntrod Uction The Nature of Enzymes LsoenzymesfjkgldjfBelum ada peringkat
- Cancer Therapy: PreclinicalDokumen8 halamanCancer Therapy: PreclinicalGeorge GeorgakisBelum ada peringkat
- DR Robert Malone Speaks OutDokumen40 halamanDR Robert Malone Speaks OutB100% (2)