Anda mungkin juga menyukai
- Hadir Xii O4Dokumen4 halamanHadir Xii O4Agus SusantaBelum ada peringkat
- GLOBALNYAAADokumen2 halamanGLOBALNYAAAAgus SusantaBelum ada peringkat
- Hadir Xii.o5Dokumen4 halamanHadir Xii.o5Agus SusantaBelum ada peringkat
- Hadir Xii.s1Dokumen4 halamanHadir Xii.s1Agus SusantaBelum ada peringkat
- DiscanDokumen4 halamanDiscanAgus SusantaBelum ada peringkat
- SEMESTERDokumen57 halamanSEMESTERAgus SusantaBelum ada peringkat
- Daftar hadir peserta penilaian XII O1Dokumen2 halamanDaftar hadir peserta penilaian XII O1Agus SusantaBelum ada peringkat
- Hadir Xii.o3Dokumen4 halamanHadir Xii.o3Agus SusantaBelum ada peringkat
- Daftar hadir penilaian tengah semesterDokumen10 halamanDaftar hadir penilaian tengah semesterAgus SusantaBelum ada peringkat
- Panduan Software RPP 20-21Dokumen3 halamanPanduan Software RPP 20-21Agus SusantaBelum ada peringkat
- Hadir Xii O4Dokumen4 halamanHadir Xii O4Agus SusantaBelum ada peringkat
- FISIKADokumen17 halamanFISIKAAgus SusantaBelum ada peringkat
- Hadir Xii.eDokumen4 halamanHadir Xii.eAgus SusantaBelum ada peringkat
- SEMESTERDokumen57 halamanSEMESTERAgus SusantaBelum ada peringkat
- Lembar JawabnyaDokumen1 halamanLembar JawabnyaAgus SusantaBelum ada peringkat
- Naskah Sampul 3Dokumen1 halamanNaskah Sampul 3Agus SusantaBelum ada peringkat
- Kisi - Kisi - Seleksi - PPG - Dalam - Jabatan - 2018 PDFDokumen581 halamanKisi - Kisi - Seleksi - PPG - Dalam - Jabatan - 2018 PDFrahmad08Belum ada peringkat
- LKPD ParijoDokumen15 halamanLKPD ParijoAgus SusantaBelum ada peringkat
- Latihan SoalDokumen1 halamanLatihan SoalAgus SusantaBelum ada peringkat
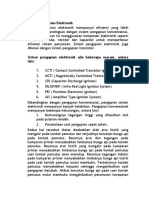
- Sistem Pengapian ElektronikDokumen3 halamanSistem Pengapian ElektronikAgus SusantaBelum ada peringkat
- RPP Kelincahan ViiiDokumen18 halamanRPP Kelincahan ViiiAgus Susanta100% (1)
- Bahan Ajar Sepak BolaDokumen6 halamanBahan Ajar Sepak BolaAgus SusantaBelum ada peringkat
- 1-Silabus Simkomdig 10-14 SMK MuhDokumen10 halaman1-Silabus Simkomdig 10-14 SMK MuhAgus SusantaBelum ada peringkat
- Pemasangan Pengujian Dan Pemeriksaan Alat Pengaman KelistrikanDokumen68 halamanPemasangan Pengujian Dan Pemeriksaan Alat Pengaman Kelistrikanmuhammadsandi100% (1)
- KKNI II Teknik Kendaraan RinganDokumen17 halamanKKNI II Teknik Kendaraan RinganDaniel Karya Teknik SteelBelum ada peringkat
- Pemasangan Pengujian Dan Pemeriksaan Alat Pengaman KelistrikanDokumen68 halamanPemasangan Pengujian Dan Pemeriksaan Alat Pengaman Kelistrikanmuhammadsandi100% (1)
- RPP Simdig 2019 - 2020Dokumen66 halamanRPP Simdig 2019 - 2020Agus Susanta67% (3)
- Pencak Silat SMKDokumen13 halamanPencak Silat SMKAgus SusantaBelum ada peringkat
- RPP BOLA VOLIDokumen42 halamanRPP BOLA VOLIAgus SusantaBelum ada peringkat