Anda mungkin juga menyukai
- Depression OutlineDokumen8 halamanDepression OutlineErica93% (15)
- Problem Management Process Ver1.0Dokumen32 halamanProblem Management Process Ver1.0drustagi100% (1)
- DepressionDokumen9 halamanDepressionErica100% (4)
- A Common Challenge in Older Adults: Classification, Overlap, and Therapy of Depression and DementiaDokumen13 halamanA Common Challenge in Older Adults: Classification, Overlap, and Therapy of Depression and DementiaDedy LeoBelum ada peringkat
- Goldberg Depression Test ScoresDokumen3 halamanGoldberg Depression Test ScoresBrittanyBelum ada peringkat
- Unipolar Late-Onset Depression: A ComprehensiveDokumen18 halamanUnipolar Late-Onset Depression: A ComprehensiveargatuBelum ada peringkat
- Assessment and Treatment of Major Depression in Older AdultsDokumen7 halamanAssessment and Treatment of Major Depression in Older AdultsNelson GuerraBelum ada peringkat
- 2020 Nemeroff - DeP ReviewDokumen15 halaman2020 Nemeroff - DeP Reviewnermal93Belum ada peringkat
- Depression in Schizophrenia: Perspective in The Era of "Atypical" Antipsychotic AgentsDokumen11 halamanDepression in Schizophrenia: Perspective in The Era of "Atypical" Antipsychotic AgentsAhmad RayanBelum ada peringkat
- Clinical Practice Guidelines For Management of Depression in ElderlyDokumen36 halamanClinical Practice Guidelines For Management of Depression in ElderlyAlbghdadi CristianBelum ada peringkat
- Epidemiology: Figures 2.1 2.2Dokumen3 halamanEpidemiology: Figures 2.1 2.2yoongiBelum ada peringkat
- Depression in The Elderly: Clinical Features and Risk FactorsDokumen7 halamanDepression in The Elderly: Clinical Features and Risk FactorsJulius Martin SiagianBelum ada peringkat
- CPG-GtiPsy 10Dokumen100 halamanCPG-GtiPsy 10Ursache BogdanBelum ada peringkat
- Depression Among Older Adults: A 20-Year Update On Five Common Myths and MisconceptionsDokumen16 halamanDepression Among Older Adults: A 20-Year Update On Five Common Myths and MisconceptionsLucia EmanuelaBelum ada peringkat
- Affective Disorders and Risk of Developing Dementia Systematic ReviewDokumen10 halamanAffective Disorders and Risk of Developing Dementia Systematic ReviewMaría-Paz Acevedo DiazBelum ada peringkat
- Appi Focus 20160036Dokumen7 halamanAppi Focus 20160036Dewi NofiantiBelum ada peringkat
- Manejo de Depresion en EMDokumen17 halamanManejo de Depresion en EMAngela Villazon CriolloBelum ada peringkat
- Poststroke Depression: A ReviewDokumen9 halamanPoststroke Depression: A ReviewSnehaBelum ada peringkat
- The Complexity of The Relationship Between "Dementia" and DepressionDokumen3 halamanThe Complexity of The Relationship Between "Dementia" and DepressionPeertechz Publications Inc.Belum ada peringkat
- Depresion Geronte 2022Dokumen14 halamanDepresion Geronte 2022Paul CastañedaBelum ada peringkat
- A CONCISE REVIEW ON DEPRESSION AND ALTERNATIVE THERAPIESDari EverandA CONCISE REVIEW ON DEPRESSION AND ALTERNATIVE THERAPIESBelum ada peringkat
- Research and Treatment Approaches To Depression: Cite This PaperDokumen10 halamanResearch and Treatment Approaches To Depression: Cite This PaperSnehaBelum ada peringkat
- Dysthymia: More Than Minor DepressionDokumen6 halamanDysthymia: More Than Minor DepressionMasithaBelum ada peringkat
- Depression: Lezan Marewan MhammadDokumen8 halamanDepression: Lezan Marewan MhammadDlzar AbubakrBelum ada peringkat
- Depresion JurnalDokumen10 halamanDepresion JurnalPaskalia ChristinBelum ada peringkat
- Depression Types, Causes, Symptoms, Risk Factor, and TreatmentDokumen7 halamanDepression Types, Causes, Symptoms, Risk Factor, and TreatmentEditor IJTSRDBelum ada peringkat
- Husain Krautter 2021 Late Life Depression The EssentialsDokumen12 halamanHusain Krautter 2021 Late Life Depression The EssentialscarolinaBelum ada peringkat
- Cognición en La DepresiónDokumen5 halamanCognición en La DepresiónLLita LLitolaBelum ada peringkat
- Psychiatric Disorders in The ElderlyDokumen11 halamanPsychiatric Disorders in The ElderlyribkaBelum ada peringkat
- Assessment of Childhood Depression: Allan Chrisman, Helen Egger, Scott N. Compton, John Curry & David B. GoldstonDokumen7 halamanAssessment of Childhood Depression: Allan Chrisman, Helen Egger, Scott N. Compton, John Curry & David B. Goldstonyeremias setyawanBelum ada peringkat
- The Costs of Depression - Kessler2012Dokumen14 halamanThe Costs of Depression - Kessler2012chen eliseBelum ada peringkat
- Diagnosis of Depression in Elderly PatientsDokumen8 halamanDiagnosis of Depression in Elderly PatientsJosé Jair Campos ReisBelum ada peringkat
- Depression in Children and AdolescentsDokumen16 halamanDepression in Children and AdolescentsAvimar JuniorBelum ada peringkat
- Major Depression in Primary Care JOURNAL READINGDokumen18 halamanMajor Depression in Primary Care JOURNAL READINGAditya Chandra ForestaBelum ada peringkat
- Alladin Cogn Hypnther4deprDokumen174 halamanAlladin Cogn Hypnther4deprssorin_444100% (1)
- Clinical Practice Guidelines For Management of Depression in ElderlyDokumen22 halamanClinical Practice Guidelines For Management of Depression in ElderlyAmalina Elvira AnggrainiBelum ada peringkat
- Stuck in A Rut: Rethinking Depression and Its Treatment: Paul E. Holtzheimer and Helen S. MaybergDokumen9 halamanStuck in A Rut: Rethinking Depression and Its Treatment: Paul E. Holtzheimer and Helen S. MaybergIlias MaBelum ada peringkat
- DepressionDokumen25 halamanDepressionVani Jain0% (2)
- Depression in The Elderly: Clinical PracticeDokumen9 halamanDepression in The Elderly: Clinical PracticejpenasotoBelum ada peringkat
- Depression Research Paper PDFDokumen8 halamanDepression Research Paper PDFgz9g97ha100% (1)
- Dysthymia More Than "Minor" DepressionDokumen5 halamanDysthymia More Than "Minor" DepressionNathaly BerríoBelum ada peringkat
- Review Affective Disorders and Risk of Developing Dementia: SystematicDokumen11 halamanReview Affective Disorders and Risk of Developing Dementia: SystematicSi Se Puede NomasfotomultasBelum ada peringkat
- Predicting Bipolar Disorder On The Basis of Phenomenology Implications For Prevention and Early InterventionDokumen16 halamanPredicting Bipolar Disorder On The Basis of Phenomenology Implications For Prevention and Early InterventionEmiBelum ada peringkat
- Rao Chen 2009. DialoguesClinNeurosci-11-45Dokumen18 halamanRao Chen 2009. DialoguesClinNeurosci-11-45Javiera Luna Marcel Zapata-SalazarBelum ada peringkat
- Depression in AdolescenceDokumen12 halamanDepression in AdolescenceAnonymous zxTFUoqzklBelum ada peringkat
- Lehtinen 1994Dokumen4 halamanLehtinen 1994HARINI KBelum ada peringkat
- Depressive Symptoms Are Prevalent in Childhood-Onset Systemic Lupus Erythematosus (cSLE)Dokumen9 halamanDepressive Symptoms Are Prevalent in Childhood-Onset Systemic Lupus Erythematosus (cSLE)Random PersonBelum ada peringkat
- Case Study MASTERSDokumen7 halamanCase Study MASTERSAnuja KumariBelum ada peringkat
- Feb 6 Introd Results Disc GPSY 513 Research Paper References AbstractDokumen6 halamanFeb 6 Introd Results Disc GPSY 513 Research Paper References AbstractEva MartinBelum ada peringkat
- Cureus 0009 00000001813Dokumen3 halamanCureus 0009 00000001813Yeray GranadoBelum ada peringkat
- Depression ResearchDokumen1 halamanDepression ResearchKlare MillerBelum ada peringkat
- Comorbid Depression in Medical DiseasesDokumen22 halamanComorbid Depression in Medical DiseasesArmando Marín FloresBelum ada peringkat
- Myocardial Infarction and Depression: A Review Article: Reza Bagherian-Sararoudi, Hamid Sanei, Ali BaghbanianDokumen7 halamanMyocardial Infarction and Depression: A Review Article: Reza Bagherian-Sararoudi, Hamid Sanei, Ali BaghbanianT SeriesBelum ada peringkat
- Autism Characteristics in Older Adults With Depressive DisordersDokumen9 halamanAutism Characteristics in Older Adults With Depressive DisordersKharisma FatwasariBelum ada peringkat
- Depression in Cognitive ImpairmentDokumen8 halamanDepression in Cognitive ImpairmentAnais UrdanetaBelum ada peringkat
- Major Depressive Disorder in Children and Adolescents: Sandra Mullen, Pharmd, BCPPDokumen9 halamanMajor Depressive Disorder in Children and Adolescents: Sandra Mullen, Pharmd, BCPPbogdancoticaBelum ada peringkat
- Untitled 7Dokumen11 halamanUntitled 7Ishita AdhikariBelum ada peringkat
- Age, Aging, and Mental HealthDokumen21 halamanAge, Aging, and Mental HealthTulaBelum ada peringkat
- Profil Lanjut Usia Dengan Depresi Yang Tinggal Di Balai Penyantunan Lanjut Usia Senja Cerah ManadoDokumen9 halamanProfil Lanjut Usia Dengan Depresi Yang Tinggal Di Balai Penyantunan Lanjut Usia Senja Cerah ManadofaeBelum ada peringkat
- Dealing with Depression: A commonsense guide to mood disordersDari EverandDealing with Depression: A commonsense guide to mood disordersPenilaian: 2 dari 5 bintang2/5 (1)
- Schizophrenia: A Guide to the Symptoms, Management, and Treatment of SchizophreniaDari EverandSchizophrenia: A Guide to the Symptoms, Management, and Treatment of SchizophreniaBelum ada peringkat
- Health Design Thinking An Innovative Approach in PDokumen6 halamanHealth Design Thinking An Innovative Approach in PElena AlnaderBelum ada peringkat
- E Book PerformanceDokumen396 halamanE Book PerformanceAnkur DhirBelum ada peringkat
- Articles Training GuideDokumen156 halamanArticles Training GuidescribdgiridarBelum ada peringkat
- Jamila Chapter 2 and 3 With CorrectionsDokumen18 halamanJamila Chapter 2 and 3 With CorrectionsFAGAS FoundationBelum ada peringkat
- Assignment Set No. 3 - Nieva O. MairinaDokumen6 halamanAssignment Set No. 3 - Nieva O. MairinaNieva MairinaBelum ada peringkat
- Attendance - CE - OverallDokumen12 halamanAttendance - CE - Overallshashikant chitranshBelum ada peringkat
- Modified Double Glove TechniqueDokumen1 halamanModified Double Glove TechniqueSohaib NawazBelum ada peringkat
- Catchup Math - Grade 72Dokumen3 halamanCatchup Math - Grade 72MARINELIA CLAMOSA100% (1)
- Purposive Communications 2 Notes 6Dokumen5 halamanPurposive Communications 2 Notes 6Gilyn NaputoBelum ada peringkat
- CHAPTER1Dokumen31 halamanCHAPTER1jinscollantesBelum ada peringkat
- Anurag Goel: Principal, Business Consulting and Advisory at SAP (Among Top 0.2% Global SAP Employees)Dokumen5 halamanAnurag Goel: Principal, Business Consulting and Advisory at SAP (Among Top 0.2% Global SAP Employees)tribendu7275Belum ada peringkat
- Polytechnic LecturerDokumen4 halamanPolytechnic LecturersambhudharmadevanBelum ada peringkat
- 2008 AM MinutesDokumen112 halaman2008 AM MinutesjesseBelum ada peringkat
- CircularVaccnies 01032024Dokumen3 halamanCircularVaccnies 01032024bidafo2019Belum ada peringkat
- Unit Outline: School of Biomedical Biomolecular and Chemical SciencesDokumen4 halamanUnit Outline: School of Biomedical Biomolecular and Chemical SciencesEvilasio CostaBelum ada peringkat
- Literature ReviewDokumen6 halamanLiterature Reviewapi-609322356Belum ada peringkat
- 0 Title 1Dokumen12 halaman0 Title 1RODJHEN ANNE P. BARQUILLABelum ada peringkat
- 6 A Lesson 4 - Compare and Contrast RocksDokumen3 halaman6 A Lesson 4 - Compare and Contrast Rocksapi-242291532100% (1)
- tws-4 AssessmentDokumen5 halamantws-4 Assessmentapi-284346424Belum ada peringkat
- Practical ResearchDokumen33 halamanPractical ResearchMonica SibayanBelum ada peringkat
- Human Resources Development Adaro Group Subject Application For Job OpportunityDokumen18 halamanHuman Resources Development Adaro Group Subject Application For Job OpportunityWilly Haryo KusumoBelum ada peringkat
- Press Release Brainly in The PhilippinesDokumen1 halamanPress Release Brainly in The PhilippinesGiancarlo Muñoz ViterboBelum ada peringkat
- Sim Isso É IncrivelDokumen3 halamanSim Isso É IncrivelRenan RezendeBelum ada peringkat
- Program Evaluation RubricDokumen13 halamanProgram Evaluation RubricShea HurstBelum ada peringkat
- There Is More Intellect Than Emotions in Our Way of Life - DebateDokumen2 halamanThere Is More Intellect Than Emotions in Our Way of Life - DebateMrinal Tripathi0% (1)
- School Culture and Its Relationship With Teacher LeadershipDokumen15 halamanSchool Culture and Its Relationship With Teacher LeadershipCarmela BorjayBelum ada peringkat
- Child Support For Adult ChildrenDokumen12 halamanChild Support For Adult ChildrenBantug De Ocampo JinkeeBelum ada peringkat
- Applicationform Draft Print For AllDokumen3 halamanApplicationform Draft Print For AllShankha Suvra Mondal ChatterjeeBelum ada peringkat
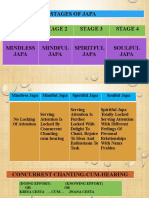
- SOULFUL JAPA - Bliss Unlimited by Japa YagnaDokumen28 halamanSOULFUL JAPA - Bliss Unlimited by Japa Yagnabalaganesh spk100% (1)