Anda mungkin juga menyukai
- Nfpa 791-R2024Dokumen20 halamanNfpa 791-R2024Ivan MarquezBelum ada peringkat
- HCF Mid ExtrasDokumen3 halamanHCF Mid Extrasnoneother2Belum ada peringkat
- Mba Resource 13-14Dokumen102 halamanMba Resource 13-14saksham23Belum ada peringkat
- Terminology For Implant Prostheses PDFDokumen5 halamanTerminology For Implant Prostheses PDFHugoMoralesTecnicoDentalBelum ada peringkat
- Human Factors and Safety Culture in Maritime Safety (Revised)Dokumen10 halamanHuman Factors and Safety Culture in Maritime Safety (Revised)Al-aayan D. IsmaelBelum ada peringkat
- Professional Teacher - Secondary (Social Studies) - 03-2024Dokumen45 halamanProfessional Teacher - Secondary (Social Studies) - 03-2024PRC BaguioBelum ada peringkat
- 3-PHAP vs. Secretary of Health (Domer)Dokumen5 halaman3-PHAP vs. Secretary of Health (Domer)Arnel ManalastasBelum ada peringkat
- Botswana Ref Ranges PaperDokumen7 halamanBotswana Ref Ranges PaperMunyaradzi MangwendezaBelum ada peringkat
- 2017 DgldmetDokumen5 halaman2017 DgldmetLucas FrançaBelum ada peringkat
- Cigna Dental Care Patient Charge Schedule: (Dhmo)Dokumen16 halamanCigna Dental Care Patient Charge Schedule: (Dhmo)Susanta BeheraBelum ada peringkat
- An Extras Cover For A Healthier LifestyleDokumen6 halamanAn Extras Cover For A Healthier LifestylealterchicBelum ada peringkat
- Unitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageDokumen9 halamanUnitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageAdam CliftonBelum ada peringkat
- Super ExtrasDokumen8 halamanSuper ExtrasPloverBelum ada peringkat
- Covered Services Network Plan Pays Benefit Guidelines Non-Network Plan PaysDokumen2 halamanCovered Services Network Plan Pays Benefit Guidelines Non-Network Plan PaysJohnny CallananBelum ada peringkat
- PMW 0031 2.19 PDFDokumen13 halamanPMW 0031 2.19 PDFFelton Small Jr.Belum ada peringkat
- Everyday Extras: Get The Same Amount Back Each Time You VisitDokumen2 halamanEveryday Extras: Get The Same Amount Back Each Time You Visitfrank.wangBelum ada peringkat
- 2010 UHC Medical Plan ComparisonDokumen2 halaman2010 UHC Medical Plan Comparisonapi-20618861Belum ada peringkat
- Unitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageDokumen1 halamanUnitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageAdam CliftonBelum ada peringkat
- Costing Exercise - SHDokumen16 halamanCosting Exercise - SHSoe HtikeBelum ada peringkat
- Gyll Aaron Insurance Verification 1654900113Dokumen2 halamanGyll Aaron Insurance Verification 1654900113Jean Alyssa Mae CalingacionBelum ada peringkat
- 2019 Plan BenefitsDokumen14 halaman2019 Plan BenefitsMichelleJeungBelum ada peringkat
- Premier 2000 NWDokumen2 halamanPremier 2000 NWacolyteBelum ada peringkat
- BenefitBrochure - 2021-08-18 15 - 26 - 56Dokumen13 halamanBenefitBrochure - 2021-08-18 15 - 26 - 56MJ SkyBelum ada peringkat
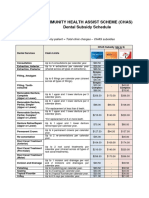
- CHAS Dental Subsidy ScheduleDokumen1 halamanCHAS Dental Subsidy ScheduleEugeneBelum ada peringkat
- Dental PPO30 - 2017Dokumen2 halamanDental PPO30 - 2017SporkleBelum ada peringkat
- HCF Starter Extras (With Optical) : Product SummaryDokumen3 halamanHCF Starter Extras (With Optical) : Product SummaryAlyssa LBelum ada peringkat
- Aflac Advantage Plan Benefit Summary 5.20Dokumen7 halamanAflac Advantage Plan Benefit Summary 5.20Mary MurphyBelum ada peringkat
- Generic Open Enrollment KitDokumen22 halamanGeneric Open Enrollment KitSteve BarrowsBelum ada peringkat
- Snap Guardian Dental Plan Summary 2022Dokumen4 halamanSnap Guardian Dental Plan Summary 2022Samson FungBelum ada peringkat
- EyeMed Benefit Plan SummaryDokumen2 halamanEyeMed Benefit Plan SummaryNestor Fabian Bermudez ZuletaBelum ada peringkat
- Pinkerten - Reed (4,000lbp) / Etinger, Zotano, Bacon XDokumen1 halamanPinkerten - Reed (4,000lbp) / Etinger, Zotano, Bacon XNassif Abi AbdallahBelum ada peringkat
- 10x45 Bargain Hunter - Value Stock Screening Report, January 2010Dokumen21 halaman10x45 Bargain Hunter - Value Stock Screening Report, January 2010The Manual of IdeasBelum ada peringkat
- Hygeia HMO SME Plans Proposal - 2022 - FinalDokumen4 halamanHygeia HMO SME Plans Proposal - 2022 - FinalBanks C. GeorgeBelum ada peringkat
- Benefit at A GlanceDokumen2 halamanBenefit at A GlanceShiv ChauhanBelum ada peringkat
- Evident Design Pricing Sept 2020 - LABSDokumen1 halamanEvident Design Pricing Sept 2020 - LABSHunterBelum ada peringkat
- Bup I36 Sbcu20Dokumen1 halamanBup I36 Sbcu20Condee TeerakBelum ada peringkat
- Women's Reproductive Health Free Clinic: Personnel ExpensesDokumen2 halamanWomen's Reproductive Health Free Clinic: Personnel ExpensesHujale MaxamedBelum ada peringkat
- Dental Plans and Rates: Bay AreaDokumen6 halamanDental Plans and Rates: Bay AreaJDanaBelum ada peringkat
- Australian Schedule and Dental Glossary 13th EditionDokumen100 halamanAustralian Schedule and Dental Glossary 13th EditionAmethystVonBelum ada peringkat
- Brochure - EZCare (Nov 2022)Dokumen11 halamanBrochure - EZCare (Nov 2022)Darren ChenBelum ada peringkat
- ProductsDokumen3 halamanProductsYaseenBelum ada peringkat
- Will "Periodontal Treatments" Be Applied? Y/N: "This Is The Optimal "Dental Treatment Plan" For Your Case"Dokumen7 halamanWill "Periodontal Treatments" Be Applied? Y/N: "This Is The Optimal "Dental Treatment Plan" For Your Case"Rami aldobehBelum ada peringkat
- HPA00001134392 Mansfield PAC 3557 HP 1625 Coverage Selection FormDokumen7 halamanHPA00001134392 Mansfield PAC 3557 HP 1625 Coverage Selection FormLinda MansfieldBelum ada peringkat
- Dental PPO20 - 2017Dokumen2 halamanDental PPO20 - 2017SporkleBelum ada peringkat
- Pet Care PlanDokumen1 halamanPet Care PlanAnonymous ZgY35hGBelum ada peringkat
- Khedekar Tejas - 2017003609 Manish Kalwar - 2017003770: Hangover HelpersDokumen1 halamanKhedekar Tejas - 2017003609 Manish Kalwar - 2017003770: Hangover HelperstejasBelum ada peringkat
- 價目表 Price List: CON/PL-02Dokumen1 halaman價目表 Price List: CON/PL-02Victor IpBelum ada peringkat
- Young Adult BrochureDokumen5 halamanYoung Adult BrochureahsanBelum ada peringkat
- Eye Med SummaryDokumen2 halamanEye Med SummaryparthaBelum ada peringkat
- LCCWorksheet - XLSX SafeDokumen10 halamanLCCWorksheet - XLSX SafeshittiestheadBelum ada peringkat
- Aetna Dental High DmoDokumen5 halamanAetna Dental High DmoBeau PeskaBelum ada peringkat
- Pet Insurance ComparisonsDokumen2 halamanPet Insurance ComparisonsHSVC50% (2)
- Primary Care Woundcare Formulary Final Version January 2020Dokumen21 halamanPrimary Care Woundcare Formulary Final Version January 2020Dr Purva PaiBelum ada peringkat
- Amount Income Frequency Frequency X Amount Annual Budget: NotesDokumen8 halamanAmount Income Frequency Frequency X Amount Annual Budget: NotesMargaretBelum ada peringkat
- 2012 ENGINE PERFORMANCE Mode 6 - Acura PDFDokumen19 halaman2012 ENGINE PERFORMANCE Mode 6 - Acura PDFsoftallBelum ada peringkat
- Unlimited 5lkDokumen2 halamanUnlimited 5lkHashan SandeepaBelum ada peringkat
- Globalcare Health Plan Benefits ScheduleDokumen7 halamanGlobalcare Health Plan Benefits ScheduleIrwanto AyongBelum ada peringkat
- Your Benefits As of 02/09/2021: Group: Aetna Medicare HmoDokumen3 halamanYour Benefits As of 02/09/2021: Group: Aetna Medicare HmoEmily dolcettBelum ada peringkat
- The Essential Plan Chart WnyDokumen1 halamanThe Essential Plan Chart WnyJavier GramajoBelum ada peringkat
- Disclaimer: Trinet Is The Single-Employer Sponsor of All Its Benefit Plans. This Communication Is For Informational PurposesDokumen26 halamanDisclaimer: Trinet Is The Single-Employer Sponsor of All Its Benefit Plans. This Communication Is For Informational PurposesJosh JasperBelum ada peringkat
- Health & Dental Handout JUN17Dokumen2 halamanHealth & Dental Handout JUN17Darius YangBelum ada peringkat
- Wa0000.Dokumen4 halamanWa0000.Mahalaxmi AgenciesBelum ada peringkat
- 2014 Final Exam SolutionsDokumen6 halaman2014 Final Exam SolutionsAyaan Ahaan Malik-WilliamsBelum ada peringkat
- Brighter Smiles For The Masses - Colgate vs. P&G - Group 10Dokumen10 halamanBrighter Smiles For The Masses - Colgate vs. P&G - Group 10sneha upadhyayBelum ada peringkat
- 2013 CA Dental OverviewDokumen6 halaman2013 CA Dental OverviewsvlimBelum ada peringkat
- IB Comp Survey - May 2018Dokumen19 halamanIB Comp Survey - May 2018saksham23Belum ada peringkat
- ApplicationDisclosureVariable 10 YearDokumen2 halamanApplicationDisclosureVariable 10 Yearsaksham23Belum ada peringkat
- Coastal Federal Loan - TermsDokumen1 halamanCoastal Federal Loan - Termssaksham23Belum ada peringkat
- A Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125Dokumen9 halamanA Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125PREJA PATELBelum ada peringkat
- Talent MappingDokumen18 halamanTalent MappingSoumya RanjanBelum ada peringkat
- SD BIOLINE HIV 12 3.0 BrochureDokumen2 halamanSD BIOLINE HIV 12 3.0 BrochureDina Friance ManihurukBelum ada peringkat
- Introduction and Analytical Report PDFDokumen111 halamanIntroduction and Analytical Report PDFJoão Pedro GarciaBelum ada peringkat
- Statement of PurposeDokumen5 halamanStatement of PurposesagvekarpoojaBelum ada peringkat
- Effect of A Physiotherapy Program in Women With Primary DysmenorrheaDokumen6 halamanEffect of A Physiotherapy Program in Women With Primary DysmenorrheaPaula RangelBelum ada peringkat
- Gefico Maritime SectorDokumen28 halamanGefico Maritime SectorAugustine Dharmaraj100% (1)
- Karakteristik Penderita Mioma Uteri Di Rsup Prof. Dr. R.D. Kandou ManadoDokumen6 halamanKarakteristik Penderita Mioma Uteri Di Rsup Prof. Dr. R.D. Kandou ManadoIsma RotinBelum ada peringkat
- Homeopathic Remedy Pictures Alexander Gothe Julia Drinnenberg.04000 1Dokumen6 halamanHomeopathic Remedy Pictures Alexander Gothe Julia Drinnenberg.04000 1BhargavaBelum ada peringkat
- HBN 00-09 Infection ControlDokumen47 halamanHBN 00-09 Infection ControlAntenehBelum ada peringkat
- Operation Management ReportDokumen12 halamanOperation Management ReportMuntaha JunaidBelum ada peringkat
- A Beauty 671-680Dokumen29 halamanA Beauty 671-680YollyBelum ada peringkat
- Definition of Physical EducationDokumen7 halamanDefinition of Physical EducationRose Jane BangisBelum ada peringkat
- Accuracy of The Demirjian and Willems MethodsDokumen8 halamanAccuracy of The Demirjian and Willems MethodsProfessor T. A. EsanBelum ada peringkat
- 3.3.2.4 Love AnimalDokumen8 halaman3.3.2.4 Love AnimalRina ErnawatiBelum ada peringkat
- CRANE SIGNAL PERSON TRAINING SlidesDokumen73 halamanCRANE SIGNAL PERSON TRAINING SlidesAayush Agrawal100% (1)
- Cbse Term 1 Final Exam Instructions 2021-21Dokumen9 halamanCbse Term 1 Final Exam Instructions 2021-21Eshaan123thebestBelum ada peringkat
- Mental Health in The Time of Pandemic Ma. Grace Baquiran-Sison, MD, DpcomDokumen32 halamanMental Health in The Time of Pandemic Ma. Grace Baquiran-Sison, MD, Dpcomcelica juabanBelum ada peringkat
- Milk Supply Chain Management Upstream Downstream IssuesDokumen25 halamanMilk Supply Chain Management Upstream Downstream IssuesbikramBelum ada peringkat
- Satvik DietDokumen3 halamanSatvik DietDisha TBelum ada peringkat
- Play Therapy FinalDokumen8 halamanPlay Therapy FinalChandru KowsalyaBelum ada peringkat
- Men's Health US - May-June 2023Dokumen96 halamanMen's Health US - May-June 2023albertomnm900Belum ada peringkat
- The CSI Effect - Google FormsDokumen12 halamanThe CSI Effect - Google FormsZivi DegenBelum ada peringkat
- Statistical EstimationDokumen37 halamanStatistical EstimationAmanuel MaruBelum ada peringkat