Anda mungkin juga menyukai
- ASCPi - Recall 4.Dokumen287 halamanASCPi - Recall 4.Joan Ruvia Cabiscuelas AnisBelum ada peringkat
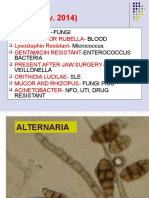
- Recall (Nov. 2014) : - Fungi Blood Micrococcus - Enterococcus Bacteria Veillonella SLE Fungi Pics Nfo, Uti, Drug ResistantDokumen79 halamanRecall (Nov. 2014) : - Fungi Blood Micrococcus - Enterococcus Bacteria Veillonella SLE Fungi Pics Nfo, Uti, Drug Resistantpcyeol67% (3)
- Urinalysis and Body Fluids for Cls & MltDari EverandUrinalysis and Body Fluids for Cls & MltBelum ada peringkat
- Recalls. 2019 AscpDokumen2 halamanRecalls. 2019 AscpJoanna Carel Lopez50% (2)
- Medical Laboratory Technician: Passbooks Study GuideDari EverandMedical Laboratory Technician: Passbooks Study GuideBelum ada peringkat
- ASCP Recall 30-08-2018 Sujan BarmanDokumen1 halamanASCP Recall 30-08-2018 Sujan BarmanLou Joseff Milan BaluyotBelum ada peringkat
- Recall Ascp MirobiologyDokumen7 halamanRecall Ascp MirobiologyNeal Allen100% (5)
- Ascp Boc QuestionsDokumen5 halamanAscp Boc QuestionsZylene Betanio Gabriel100% (4)
- Ascpi (MLS) Study Guide: Cushing's DiseaseDokumen2 halamanAscpi (MLS) Study Guide: Cushing's DiseaseCatherine Nicolas100% (5)
- ASCP-RECALLS-Compiled - Alice 2017Dokumen18 halamanASCP-RECALLS-Compiled - Alice 2017Princess Dianne Gonzaga Mendola89% (9)
- Ascp Boc QuestionsDokumen4 halamanAscp Boc QuestionsRose jane TambasenBelum ada peringkat
- Ascp Recalls (File Grabbed)Dokumen3 halamanAscp Recalls (File Grabbed)KL Suazo78% (9)
- Recall 3Dokumen22 halamanRecall 3Christine Rodriguez-Guerrero100% (4)
- As CP RecallDokumen15 halamanAs CP RecallJoanna Carel Lopez100% (2)
- January 2019 Acspi RecallsDokumen2 halamanJanuary 2019 Acspi RecallsMykeeFonelleraTanduyan50% (2)
- Recall Ascp MirobiologyDokumen7 halamanRecall Ascp MirobiologyJie Fuentes80% (5)
- TH ST NDDokumen3 halamanTH ST NDDarlene Evangelista100% (1)
- AscpDokumen1 halamanAscpGerald John Paz0% (5)
- MLS-ASCPi-Recalls REVISEDDokumen11 halamanMLS-ASCPi-Recalls REVISEDAstrud Labrador100% (3)
- Recalls WordsologyDokumen25 halamanRecalls WordsologyJie Fuentes91% (11)
- Ascpi Recalls 2016Dokumen9 halamanAscpi Recalls 2016Zylene Gabriel100% (1)
- ASCP ReviewerDokumen8 halamanASCP Reviewergillian102290100% (6)
- Ascp Pointers MicroDokumen73 halamanAscp Pointers Microraica56_362842087100% (6)
- ASCPi Recall Questions Gio 1Dokumen7 halamanASCPi Recall Questions Gio 1Joanna Carel Lopez100% (4)
- Recalls ASCPDokumen6 halamanRecalls ASCPAstrud Labrador100% (5)
- Hema PointrDokumen4 halamanHema PointrLeonida DalugdogBelum ada peringkat
- ASCP Questions (Autosaved) - 1Dokumen56 halamanASCP Questions (Autosaved) - 1Glenn Perez100% (16)
- Ascp PointersDokumen78 halamanAscp PointersNIMKY EMBER B. CLAMOHOY100% (14)
- ASCP Recalls 5Dokumen9 halamanASCP Recalls 5Cristina Vergel De DiosBelum ada peringkat
- ASCP RecallsDokumen4 halamanASCP RecallsKaren SantiagoBelum ada peringkat
- Compre ASCP Part 2Dokumen20 halamanCompre ASCP Part 2Deanna Lepon67% (3)
- Study Stack - M (ASCP) EXAM Table Review PDFDokumen9 halamanStudy Stack - M (ASCP) EXAM Table Review PDF장주연100% (2)
- ASCP Recalls 2017-2018 Flashcards - Quizlet - AmgadDokumen80 halamanASCP Recalls 2017-2018 Flashcards - Quizlet - AmgadShiv Prajapati100% (17)
- MLS ASCP Study Guide PDFDokumen2 halamanMLS ASCP Study Guide PDFyowubhatori100% (2)
- Invalid Prolonged Results May Result When The Hematocrit Exceeds 55%Dokumen15 halamanInvalid Prolonged Results May Result When The Hematocrit Exceeds 55%asma100% (3)
- Your BOC Exam: What You Need To Know To Be ReadyDokumen35 halamanYour BOC Exam: What You Need To Know To Be ReadyDeanne Lamban100% (3)
- ASCP Recalls As of August' 2013: Ionized CalciumDokumen22 halamanASCP Recalls As of August' 2013: Ionized Calciumbaihern24Belum ada peringkat
- August 03 2017 Recalls Mls (Ascpi)Dokumen6 halamanAugust 03 2017 Recalls Mls (Ascpi)Joanna Carel Lopez100% (3)
- ASCPDokumen5 halamanASCPDjdjjd Siisus100% (3)
- Ascp PointersDokumen78 halamanAscp Pointersbaihern2450% (2)
- Haematology Ascp RecallDokumen7 halamanHaematology Ascp RecallMona AliBelum ada peringkat
- BOC 5th Edition CalculationsDokumen3 halamanBOC 5th Edition Calculationsthrowawy75% (4)
- BOC Study Guide Errata 09082010Dokumen42 halamanBOC Study Guide Errata 09082010D.L67% (3)
- MLS ASCP Exam Recall Questions Flashcards - QuizletDokumen8 halamanMLS ASCP Exam Recall Questions Flashcards - Quizletyeliz kurt100% (3)
- Immunohematology HandoutDokumen9 halamanImmunohematology Handoutmarkylopez2383% (6)
- FEB 2017 RecallsDokumen2 halamanFEB 2017 RecallsLucid LynxBelum ada peringkat
- Blood BankingDokumen5 halamanBlood BankingTel LyBelum ada peringkat
- Clinical ChemistryDokumen10 halamanClinical ChemistryChristina AtefBelum ada peringkat
- RecallsDokumen1 halamanRecallsTinay100% (1)
- AABB 2021 Blood Bank Fundamentals Course SBB/BB Exam Review: Supplemental HandoutDokumen51 halamanAABB 2021 Blood Bank Fundamentals Course SBB/BB Exam Review: Supplemental HandoutDyne Sabijon100% (1)
- Simulated No.1 General Rule:: ExceptDokumen29 halamanSimulated No.1 General Rule:: ExceptJie FuentesBelum ada peringkat
- Exam Recalls - WordsologyDokumen200 halamanExam Recalls - WordsologyShiv Prajapati83% (29)
- MLS ASCPi Exam Content Guidlines 2019Dokumen12 halamanMLS ASCPi Exam Content Guidlines 2019Islam100% (2)
- ASCP ExamDokumen10 halamanASCP Examnoone100% (3)
- BB NotesDokumen5 halamanBB NotesFait HeeBelum ada peringkat
- Immuno For ASCP ReviewDokumen25 halamanImmuno For ASCP ReviewWl SorianoBelum ada peringkat
- Virology ASCPDokumen24 halamanVirology ASCP2131443Belum ada peringkat
- MUST To KNOW in Immunohematology Blood BankingDokumen18 halamanMUST To KNOW in Immunohematology Blood BankingDanielJeremy DelaCruz Paragas79% (14)
- Yousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Dokumen147 halamanYousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Amr AmalBelum ada peringkat
- Complications in Treatment of LYMEDokumen131 halamanComplications in Treatment of LYMECharles Mitchell100% (1)
- Update Stock PT KMD 14-6Dokumen46 halamanUpdate Stock PT KMD 14-6rio1995Belum ada peringkat
- SPIROCHETES (Treponema, Borrelia and Leptospira)Dokumen4 halamanSPIROCHETES (Treponema, Borrelia and Leptospira)Muneer Al-DahbaliBelum ada peringkat
- Snap 4dx Plus Sensitivity Specificity PDFDokumen1 halamanSnap 4dx Plus Sensitivity Specificity PDFDesriwanAnggaMedicaBelum ada peringkat
- Presentation-Lyme Disease - March13Dokumen20 halamanPresentation-Lyme Disease - March13jabirBelum ada peringkat
- Therapy Planner LymeherbsDokumen42 halamanTherapy Planner Lymeherbsalba lopezBelum ada peringkat
- Controlling Ticks and Tick-Borne DiseasesDokumen12 halamanControlling Ticks and Tick-Borne Diseasesapi-3703629100% (1)
- CJS Weekly, 31 May 2010 Edition.Dokumen8 halamanCJS Weekly, 31 May 2010 Edition.CountrysideJobsBelum ada peringkat
- Meningitis Clinical PresentationDokumen10 halamanMeningitis Clinical PresentationAniwat NillakarnBelum ada peringkat
- Public Health Alert Vol 3, Issue 7Dokumen20 halamanPublic Health Alert Vol 3, Issue 7Shirley Pigott MDBelum ada peringkat
- Diseases of PenguinsDokumen7 halamanDiseases of PenguinspaulysolBelum ada peringkat
- Lyme OverviewDokumen87 halamanLyme OverviewAmanda MehallBelum ada peringkat
- Antibiotic Guidelines For SKIN AND SOFT TISSUE INFECTIONSDokumen11 halamanAntibiotic Guidelines For SKIN AND SOFT TISSUE INFECTIONSlaptopgreyBelum ada peringkat
- Nur 111 Session 22 Sas 1Dokumen8 halamanNur 111 Session 22 Sas 1Zzimply Tri Sha UmaliBelum ada peringkat
- Stock 01 Des 22Dokumen70 halamanStock 01 Des 22kaprodiS1 stikesalfatahBelum ada peringkat
- Pediatric Lyme DiseaseDokumen52 halamanPediatric Lyme DiseaseWanda BakerBelum ada peringkat
- TorchDokumen6 halamanTorchMary Jean HernaniBelum ada peringkat
- Imo SpirocheteDokumen43 halamanImo SpirocheteGelvia AwaehBelum ada peringkat
- Mahon CompileDokumen13 halamanMahon CompileSheinor Fae GalzoteBelum ada peringkat
- TCM Diagnostics Applied To Parasite-Related Disease by Laraine Crampton, MATCM, L. Ac ... PDFDokumen102 halamanTCM Diagnostics Applied To Parasite-Related Disease by Laraine Crampton, MATCM, L. Ac ... PDFMaya PelinBelum ada peringkat
- Veterinary Parasitology: Elizabeth B. Mitchell, John W. Mccall, S. Theodore Chester, Diane LarsenDokumen3 halamanVeterinary Parasitology: Elizabeth B. Mitchell, John W. Mccall, S. Theodore Chester, Diane LarsenChorrinha ChorraBelum ada peringkat
- Chapter 1 Writing2Dokumen12 halamanChapter 1 Writing2Xuan ThuyBelum ada peringkat
- 4.vector and Water Borne-DiseasesDokumen26 halaman4.vector and Water Borne-DiseasesMuhammad AsifBelum ada peringkat
- NF - DR - Concept Map - Week 11Dokumen3 halamanNF - DR - Concept Map - Week 11Kyra Bianca R. FamacionBelum ada peringkat
- Erythroderma: 3. Erythema Chronicum Migrans (ECM)Dokumen4 halamanErythroderma: 3. Erythema Chronicum Migrans (ECM)iisisiisBelum ada peringkat
- Diagnosis and Differential Diagnosis of Rheumatoid Arthritis - UpToDateDokumen20 halamanDiagnosis and Differential Diagnosis of Rheumatoid Arthritis - UpToDateDannyGutierrezBelum ada peringkat
- Maryville NURS 623 ExamDokumen14 halamanMaryville NURS 623 ExamWizzardBelum ada peringkat
- 8.5 Case AnalysisDokumen4 halaman8.5 Case AnalysisMichal VillanuevaBelum ada peringkat
- Heron Herbals: Treating Lyme DiseaseDokumen3 halamanHeron Herbals: Treating Lyme DiseaseterryvndBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 4.5 dari 5 bintang4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (35)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDari EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDPenilaian: 5 dari 5 bintang5/5 (4)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Dari EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Penilaian: 3 dari 5 bintang3/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeDari EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgePenilaian: 4.5 dari 5 bintang4.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 4 dari 5 bintang4/5 (5)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePenilaian: 2 dari 5 bintang2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDari EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesPenilaian: 4.5 dari 5 bintang4.5/5 (1412)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionDari EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionBelum ada peringkat
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (24)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsPenilaian: 5 dari 5 bintang5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDari EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsPenilaian: 4.5 dari 5 bintang4.5/5 (39)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDari EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (44)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDari EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryPenilaian: 4 dari 5 bintang4/5 (46)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDari EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifePenilaian: 4.5 dari 5 bintang4.5/5 (254)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDari EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsBelum ada peringkat
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Dari EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Penilaian: 5 dari 5 bintang5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedPenilaian: 4 dari 5 bintang4/5 (61)