Anda mungkin juga menyukai
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionDari EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 8: UrologyDari EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyPenilaian: 3 dari 5 bintang3/5 (1)
- Jurnal Geriatri Dr. BrinnaDokumen12 halamanJurnal Geriatri Dr. Brinnabrinna aninditaBelum ada peringkat
- Journal of Geriatric Medicine and Gerontology JGMG 5 070Dokumen7 halamanJournal of Geriatric Medicine and Gerontology JGMG 5 070Dilly NizaBelum ada peringkat
- Refeeding Syndrome A Literature Review KhanDokumen7 halamanRefeeding Syndrome A Literature Review Khangw060qpy100% (1)
- Hyponatremia 2015Dokumen19 halamanHyponatremia 2015gastonsaloBelum ada peringkat
- Aged Care Brochure PDFDokumen12 halamanAged Care Brochure PDFMuhammad ZubaidiBelum ada peringkat
- Pediatrics in Review. Dehydration 2015Dokumen14 halamanPediatrics in Review. Dehydration 2015Jorge Eduardo Espinoza Rios100% (2)
- Fluids SummaryDokumen3 halamanFluids Summarymicheal1960Belum ada peringkat
- Fluid Balance and Optimal Hydration Guideline For Adult InpatientsDokumen6 halamanFluid Balance and Optimal Hydration Guideline For Adult InpatientsOvidiu MCBelum ada peringkat
- DeshidratacionDokumen14 halamanDeshidratacionAlvaro Andres Flores JimenezBelum ada peringkat
- Dehydration Isonatremic, Hyponatremic, andDokumen15 halamanDehydration Isonatremic, Hyponatremic, andalfredoibcBelum ada peringkat
- Graziella Allana Serra Alves de Oliveira Olle 2018Dokumen12 halamanGraziella Allana Serra Alves de Oliveira Olle 2018Anindya Laksmi LarasatiBelum ada peringkat
- Labcomp FDokumen23 halamanLabcomp Fking peaceBelum ada peringkat
- Nutrition Noteworthy, 4 (1) Garcia, Marcela EsperanzaDokumen7 halamanNutrition Noteworthy, 4 (1) Garcia, Marcela EsperanzadidikekoBelum ada peringkat
- Deshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Dokumen6 halamanDeshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Natalia BeltranBelum ada peringkat
- Anorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateDokumen10 halamanAnorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDatethelesphol pascalBelum ada peringkat
- Journal Pre-Proof: Clinical NutritionDokumen19 halamanJournal Pre-Proof: Clinical NutritionThay SousaBelum ada peringkat
- Fluid Imbalance (NCP)Dokumen9 halamanFluid Imbalance (NCP)Putry RainismBelum ada peringkat
- GiftasupDokumen50 halamanGiftasupFizza SiddiquiBelum ada peringkat
- Electrolyte Imbalance in CKD PatientsDokumen4 halamanElectrolyte Imbalance in CKD PatientsEditor IJTSRDBelum ada peringkat
- Rajiv Gandhi University of Health Sciences, Karnataka BangaloreDokumen13 halamanRajiv Gandhi University of Health Sciences, Karnataka BangaloreFebri SuryoBelum ada peringkat
- BMJ Open 2013 RioDokumen10 halamanBMJ Open 2013 RioNindyaReBelum ada peringkat
- Myocardial and Haemodynamic Responses To Two Fluid Regimens in African Children With Severe Malnutrition and Hypovolaemic Shock (AFRIM Study)Dokumen18 halamanMyocardial and Haemodynamic Responses To Two Fluid Regimens in African Children With Severe Malnutrition and Hypovolaemic Shock (AFRIM Study)Dina AryaniBelum ada peringkat
- Transfusión en Pacientes PediatricosDokumen14 halamanTransfusión en Pacientes PediatricosAndrea Abigail ChacónBelum ada peringkat
- Ebp Summer 2014Dokumen5 halamanEbp Summer 2014api-314483635Belum ada peringkat
- Hyponatremia and Hypernatremia in The ElderlyDokumen15 halamanHyponatremia and Hypernatremia in The ElderlyStacey WoodsBelum ada peringkat
- 2019 Article 1596Dokumen9 halaman2019 Article 1596Arina FitrianiBelum ada peringkat
- Hipernatremia en UCIDokumen7 halamanHipernatremia en UCIcolo_med1077Belum ada peringkat
- Fluid and Electrolyte Management For The Surgical PatientDokumen17 halamanFluid and Electrolyte Management For The Surgical PatientFery López NavedaBelum ada peringkat
- Anorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateDokumen11 halamanAnorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateAlejandra GarcíaBelum ada peringkat
- Nutritional Status and Dietary Guidelines of Predialytic and Hemodialytic PatientsDokumen138 halamanNutritional Status and Dietary Guidelines of Predialytic and Hemodialytic PatientsAndre SanteBelum ada peringkat
- NCBI Bookshelf-Diabetes InsipidusDokumen44 halamanNCBI Bookshelf-Diabetes InsipidusDiah Pradnya ParamitaBelum ada peringkat
- ESRD Case Analysis - Group 4Dokumen34 halamanESRD Case Analysis - Group 4Sean Jeffrey J. FentressBelum ada peringkat
- Acute Alcoholic HepatitisDokumen11 halamanAcute Alcoholic HepatitisDoc_NethoBelum ada peringkat
- Fluid Challenge RevisitedDokumen5 halamanFluid Challenge RevisitedNinda DevitaBelum ada peringkat
- Assessment of Hypovolaemia in The Critically IllDokumen10 halamanAssessment of Hypovolaemia in The Critically IllrjerezrBelum ada peringkat
- Refeeding SyndromeDokumen10 halamanRefeeding SyndromeEstefany GonzalezBelum ada peringkat
- Jonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDDokumen29 halamanJonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDrifkiBelum ada peringkat
- Avoiding Common Problems Associated With Intravenous Fluid TherapyDokumen13 halamanAvoiding Common Problems Associated With Intravenous Fluid TherapyDeepak AnBelum ada peringkat
- Realimentacion UptodateDokumen9 halamanRealimentacion UptodateVerito SalazarBelum ada peringkat
- Guideline Terbaru ACLFDokumen28 halamanGuideline Terbaru ACLFNovita ApramadhaBelum ada peringkat
- CHAP 2 Edit Final (1) - DevocionDokumen10 halamanCHAP 2 Edit Final (1) - Devociontsam127Belum ada peringkat
- Protein Energy Malnutrition in CKD PatientsDokumen4 halamanProtein Energy Malnutrition in CKD PatientsEditor IJTSRDBelum ada peringkat
- Principles of Fluid Management 2015 PDFDokumen17 halamanPrinciples of Fluid Management 2015 PDFJorge DíazBelum ada peringkat
- Guidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchDokumen7 halamanGuidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchnikopkunairBelum ada peringkat
- Pi Is 0039610912000163Dokumen17 halamanPi Is 0039610912000163Hend Al-DreesBelum ada peringkat
- Medical Nutrition Therapy For Hemodialysis PatientsDokumen24 halamanMedical Nutrition Therapy For Hemodialysis Patientsraquelt_65Belum ada peringkat
- Bundle Three Hour SSC PDFDokumen14 halamanBundle Three Hour SSC PDFRodrigo RochaBelum ada peringkat
- Infectious Diarrhea AcuteDokumen14 halamanInfectious Diarrhea AcuteOktiya SariBelum ada peringkat
- Medical Surgical Fluid and Electrolytes FVD FVEDokumen7 halamanMedical Surgical Fluid and Electrolytes FVD FVEMichaelaKatrinaTrinidadBelum ada peringkat
- Art 38Dokumen9 halamanArt 38Francesca BertaccaBelum ada peringkat
- Hamsini SreeramDokumen33 halamanHamsini SreeramkalyanpavuralaBelum ada peringkat
- Acute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Dokumen11 halamanAcute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Roscheen Berg TutorBelum ada peringkat
- Capstone Final Justin IsnerDokumen21 halamanCapstone Final Justin Isnerapi-312746225Belum ada peringkat
- Department of Health, PhilippinesDokumen38 halamanDepartment of Health, PhilippinesClaribel Domingo BayaniBelum ada peringkat
- Manejo Medico Hiperpoara Primario Mayo Clinic 2007Dokumen5 halamanManejo Medico Hiperpoara Primario Mayo Clinic 2007Kenia LopezBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderDari EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderBelum ada peringkat
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDari EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesPenilaian: 4 dari 5 bintang4/5 (2)
- Gastroenterology Hospital Handbook Volume 2: Volume, #2Dari EverandGastroenterology Hospital Handbook Volume 2: Volume, #2Belum ada peringkat
- This Is Our Third Day 24/6/2020: FirstDokumen1 halamanThis Is Our Third Day 24/6/2020: FirstdaliaBelum ada peringkat
- Emilio Aguinaldo College: School of NursingDokumen2 halamanEmilio Aguinaldo College: School of NursingdaliaBelum ada peringkat
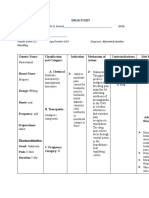
- Drug Study: - 24/june/2020Dokumen1 halamanDrug Study: - 24/june/2020daliaBelum ada peringkat
- Health Record Tracker For AdultsDokumen2 halamanHealth Record Tracker For AdultsdaliaBelum ada peringkat
- Cellulitis JournalDokumen3 halamanCellulitis JournaldaliaBelum ada peringkat
- What Is Ebola Virus DiseaseDokumen3 halamanWhat Is Ebola Virus DiseasedaliaBelum ada peringkat
- Decalcification: By: Riman Mustafa IbrahimDokumen21 halamanDecalcification: By: Riman Mustafa IbrahimdaliaBelum ada peringkat
- Hema Report PDFDokumen25 halamanHema Report PDFdaliaBelum ada peringkat
- Decalcificati ON& Dehydration: By: Riman Mustafa IbrahimDokumen21 halamanDecalcificati ON& Dehydration: By: Riman Mustafa IbrahimdaliaBelum ada peringkat
- Incident Command Education:: Biological Warfare and Biological AgentsDokumen9 halamanIncident Command Education:: Biological Warfare and Biological AgentsdaliaBelum ada peringkat
- Emilio Aguinaldo College: School of NursingDokumen1 halamanEmilio Aguinaldo College: School of NursingdaliaBelum ada peringkat
- Association Between Fluid Overload and SOFA Score Kinetics in Septic Shock Patients: A Retrospective Multicenter StudyDokumen18 halamanAssociation Between Fluid Overload and SOFA Score Kinetics in Septic Shock Patients: A Retrospective Multicenter StudydaliaBelum ada peringkat
- Assisted To Deliya Ali: - Prepared - By: Abdo Delal Ali Funcational NursesDokumen3 halamanAssisted To Deliya Ali: - Prepared - By: Abdo Delal Ali Funcational NursesdaliaBelum ada peringkat
- Acquired Immunodeficiency Syndrome (AIDS) Is A Chronic, PotentiallyDokumen13 halamanAcquired Immunodeficiency Syndrome (AIDS) Is A Chronic, PotentiallydaliaBelum ada peringkat
- Endorsement SheetDokumen2 halamanEndorsement SheetdaliaBelum ada peringkat
- Staff Development1Dokumen16 halamanStaff Development1daliaBelum ada peringkat
- Medical Center Manila - 7 Main Functional Head Nurse QuizDokumen1 halamanMedical Center Manila - 7 Main Functional Head Nurse QuizdaliaBelum ada peringkat
- New Resume 001Dokumen1 halamanNew Resume 001daliaBelum ada peringkat
- Community Organizing Participatory Action ResearchDokumen7 halamanCommunity Organizing Participatory Action ResearchdaliaBelum ada peringkat
- Emilio Aguinaldo College: School of NursingDokumen1 halamanEmilio Aguinaldo College: School of NursingdaliaBelum ada peringkat
- Journal: Nursing Leadership and ManagementDokumen9 halamanJournal: Nursing Leadership and ManagementdaliaBelum ada peringkat
- Name of Patient:: DX: Ductal Carcino MA Right Side CC: Brest Mass DATDokumen2 halamanName of Patient:: DX: Ductal Carcino MA Right Side CC: Brest Mass DATdaliaBelum ada peringkat
- Book1 PDFDokumen155 halamanBook1 PDFmantoo kumarBelum ada peringkat
- Sanaani Nur Hathi M. Nso Jugular Venous Oximetry Staff Nurse 1Dokumen7 halamanSanaani Nur Hathi M. Nso Jugular Venous Oximetry Staff Nurse 1Nur SanaaniBelum ada peringkat
- Part Time Vs Full Time Wear of Twin Block - Parekh2019Dokumen8 halamanPart Time Vs Full Time Wear of Twin Block - Parekh2019rohitBelum ada peringkat
- Tectyl Spin 10 (En-Ghs-K)Dokumen14 halamanTectyl Spin 10 (En-Ghs-K)Irna WatiBelum ada peringkat
- Basic Personality InventoryDokumen8 halamanBasic Personality InventoryElisa Mae Oranza Gura100% (1)
- Bone Marrow TransplantDokumen6 halamanBone Marrow TransplantFatihah UmerBelum ada peringkat
- ENERPEEL SA - Rev - 0 - 2011Dokumen48 halamanENERPEEL SA - Rev - 0 - 2011CHONG WEI SHENGBelum ada peringkat
- Psychophysiological Methods in NeuroscienceDokumen17 halamanPsychophysiological Methods in NeuroscienceKariela EstherBelum ada peringkat
- Dermatoscope IDS-1100: Technical Specifications Accessories & Spare PartsDokumen2 halamanDermatoscope IDS-1100: Technical Specifications Accessories & Spare PartsHemkerovner Keresztszegh von Kolowrat-KrakowskyBelum ada peringkat
- A. Mabini ST., Malate 1004 Manila, Philippines - (632) 7087701 - WWW - Bsp.gov - PH - Bspmail@bsp - Gov.phDokumen1 halamanA. Mabini ST., Malate 1004 Manila, Philippines - (632) 7087701 - WWW - Bsp.gov - PH - Bspmail@bsp - Gov.phokto namikaBelum ada peringkat
- PAGULAYAN, M - Week1ReflectionJournal109Dokumen2 halamanPAGULAYAN, M - Week1ReflectionJournal109Marimiel PagulayanBelum ada peringkat
- ORE Part 2Dokumen1 halamanORE Part 2Ruhaan AbrahamBelum ada peringkat
- DR AP - BREATHING TECHNIQUES (2020v2)Dokumen11 halamanDR AP - BREATHING TECHNIQUES (2020v2)Dr Adele PelteretBelum ada peringkat
- Clear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewDokumen4 halamanClear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Dealing With EmotionsDokumen26 halamanDealing With EmotionsAli Ijaz100% (1)
- Family Assessment 2 (Interview)Dokumen5 halamanFamily Assessment 2 (Interview)DIZZA MAE BATURIANOBelum ada peringkat
- Exploring The Factors Affecting Teacher's Effectiveness in Higher Education: An Empirical Analysis of District Gujranwala, PakistanDokumen17 halamanExploring The Factors Affecting Teacher's Effectiveness in Higher Education: An Empirical Analysis of District Gujranwala, PakistanSirajudinBelum ada peringkat
- Textbook of Pediatric Dentistry-3rd EditionDokumen18 halamanTextbook of Pediatric Dentistry-3rd EditionAnna NgBelum ada peringkat
- Do The Benefits of Medical Marijuana Justify Its LegalityDokumen4 halamanDo The Benefits of Medical Marijuana Justify Its LegalityAlexander MasakuBelum ada peringkat
- Module 1 and 2Dokumen3 halamanModule 1 and 2Leigh QuinnBelum ada peringkat
- Case Study-Eukaryotic Diversity GROUP 7Dokumen2 halamanCase Study-Eukaryotic Diversity GROUP 7Amal JosephBelum ada peringkat
- Session #38 SAS - AnaPhy (Lab)Dokumen5 halamanSession #38 SAS - AnaPhy (Lab)Cristina SottoBelum ada peringkat
- May 15, 2023 - AssignmentDokumen6 halamanMay 15, 2023 - AssignmentMARY FORTUNE MAE RAMONESBelum ada peringkat
- Ten CentersDokumen4 halamanTen CentersJohn Christopher ReguindinBelum ada peringkat
- Ophthalmology Volume 128, Issue 5 - Mai 2021Dokumen187 halamanOphthalmology Volume 128, Issue 5 - Mai 2021Fanny HazizaBelum ada peringkat
- Kuang Yeu Medical Model FrontierDokumen48 halamanKuang Yeu Medical Model FrontierSeyed Mohammad Hossein EmamiBelum ada peringkat
- PPE Inspection ChecklistDokumen5 halamanPPE Inspection ChecklistBalasubramaniamkamarajBelum ada peringkat
- Medical Clinic Standards v.1Dokumen13 halamanMedical Clinic Standards v.1ummuawisyBelum ada peringkat
- English PaperDokumen14 halamanEnglish PaperLAKSHANA KUMARAGEBelum ada peringkat
- Jurisprudance DI Questions Paper BPSC 2023 PharmapediaDokumen9 halamanJurisprudance DI Questions Paper BPSC 2023 Pharmapediakrishnamahalle12Belum ada peringkat