Anda mungkin juga menyukai
- Monitoring Mechanical Ventilation Using Ventilator WaveformsDari EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsBelum ada peringkat
- Mechanical VentilationDokumen28 halamanMechanical VentilationM BBelum ada peringkat
- Samsung Notes PDFDokumen4 halamanSamsung Notes PDFPedro Antonio Ortega BorchardtBelum ada peringkat
- Readings - Introduction To Mechanical Ventilation - Introduction To Mechanical Ventilation (10 Min) - COV19x Courseware - EdxDokumen4 halamanReadings - Introduction To Mechanical Ventilation - Introduction To Mechanical Ventilation (10 Min) - COV19x Courseware - EdxvgmanjunathBelum ada peringkat
- Pediatric Mechanical VentilationDokumen49 halamanPediatric Mechanical VentilationNirubhana ArunthavasothyBelum ada peringkat
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsDari EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouBelum ada peringkat
- Managing Mechanical VentilationDokumen7 halamanManaging Mechanical VentilationArden QuiambaoBelum ada peringkat
- Pulmonary Function Tests in Clinical PracticeDari EverandPulmonary Function Tests in Clinical PracticeAli AltalagPenilaian: 5 dari 5 bintang5/5 (1)
- Physiologic and Pathophysiologic Consequences of Mechanical Ventilation - UpToDateDokumen21 halamanPhysiologic and Pathophysiologic Consequences of Mechanical Ventilation - UpToDateacesacesBelum ada peringkat
- Basics of Mechanical VentilationDokumen5 halamanBasics of Mechanical Ventilationruhaina malikBelum ada peringkat
- Modos de Ventilación Mecánica PDFDokumen19 halamanModos de Ventilación Mecánica PDFVictor M' PimentelBelum ada peringkat
- Ventilator Settings: Ventilator Settings Are Tailored To TheDokumen7 halamanVentilator Settings: Ventilator Settings Are Tailored To Thearnol3090Belum ada peringkat
- Mechanical Ventilator.-1Dokumen11 halamanMechanical Ventilator.-1shemo hayatBelum ada peringkat
- VentilatorDokumen9 halamanVentilatorSheeba StephenBelum ada peringkat
- Asma 6Dokumen25 halamanAsma 6punkgatitBelum ada peringkat
- Mechanical Ventilation - StatPearls - NCBI BookshelfDokumen15 halamanMechanical Ventilation - StatPearls - NCBI BookshelfmohammedBelum ada peringkat
- Mechanical VentilatorsDokumen11 halamanMechanical VentilatorsIra Katrina Bernales MendozaBelum ada peringkat
- ARTventilacion Mecanica en EMDokumen3 halamanARTventilacion Mecanica en EMNicole Ivette Arias RizikBelum ada peringkat
- Ventilators, Intensive CareDokumen48 halamanVentilators, Intensive CarealetripoleBelum ada peringkat
- Mechanical VentilationDokumen52 halamanMechanical VentilationSalma Omrr100% (1)
- Ventilacion Mecanica 2008Dokumen14 halamanVentilacion Mecanica 2008Macros FitBelum ada peringkat
- Advances in Mechanical Ventilation 4AH PDFDokumen11 halamanAdvances in Mechanical Ventilation 4AH PDFsérgio_nakano_2Belum ada peringkat
- Mechanical VentilationDokumen16 halamanMechanical VentilationArt Christian Ramos88% (8)
- Clinical Science Session: OlehDokumen17 halamanClinical Science Session: OlehMira MustikaBelum ada peringkat
- Mechanical VentilationDokumen9 halamanMechanical VentilationFriends ForeverBelum ada peringkat
- Ventilator Management: Introduction To Ventilator Management, Modes of Mechanical Ventilation, Methods of Ventilatory SupportDokumen12 halamanVentilator Management: Introduction To Ventilator Management, Modes of Mechanical Ventilation, Methods of Ventilatory SupportDellBelum ada peringkat
- Physiologic and Pathophysiologic Consequences of Mechanical Ventilation - UpToDaDokumen23 halamanPhysiologic and Pathophysiologic Consequences of Mechanical Ventilation - UpToDaGia Villavicencio BoniniBelum ada peringkat
- Mechanical Ventilation in Pediatric PatientDokumen11 halamanMechanical Ventilation in Pediatric PatientHandris YanitraBelum ada peringkat
- Mechanical Ventilation SeminarDokumen82 halamanMechanical Ventilation Seminarrajan kumar90% (21)
- Mechanical VentilatorDokumen22 halamanMechanical VentilatorGurinder GillBelum ada peringkat
- High Frequency Ventilation: Level 1Dokumen24 halamanHigh Frequency Ventilation: Level 1Prashanth PrashuBelum ada peringkat
- Care of Patients With Mechanical VentilatorDokumen4 halamanCare of Patients With Mechanical VentilatorIman Bee Sanayon0% (1)
- Positive End-Expiratory Pressure and Lung ComplianDokumen6 halamanPositive End-Expiratory Pressure and Lung ComplianElfahime HamzaBelum ada peringkat
- Mechanical VentilationDokumen16 halamanMechanical VentilationBhawna JoshiBelum ada peringkat
- One Lung Ventilation: General Principles - UpToDateDokumen26 halamanOne Lung Ventilation: General Principles - UpToDateAna Belén Artero CastañoBelum ada peringkat
- Automatic Control: Radouan Ait Mouha ID:12190210101Dokumen8 halamanAutomatic Control: Radouan Ait Mouha ID:12190210101Redouan Ait MouhaBelum ada peringkat
- One Lung Ventilation - General Principles - UpToDateDokumen25 halamanOne Lung Ventilation - General Principles - UpToDatemayteveronica1000Belum ada peringkat
- Demonstration On Mechanical VentilationDokumen8 halamanDemonstration On Mechanical VentilationHimaniBelum ada peringkat
- Mechanical VentilationDokumen6 halamanMechanical Ventilationedison aorianoBelum ada peringkat
- Lung Mechncs IDokumen16 halamanLung Mechncs Iafshan.arzooBelum ada peringkat
- Wa0007.Dokumen16 halamanWa0007.Ulises CasarrubiasBelum ada peringkat
- Basic Modes of Mechanical VentilationDokumen16 halamanBasic Modes of Mechanical VentilationDoreli RuizBelum ada peringkat
- Modes of VentilatorDokumen17 halamanModes of VentilatorFahrizal MuhammadBelum ada peringkat
- Low-Tidal-Volume Ventilation in The Acute Respiratory Distress SyndromeDokumen8 halamanLow-Tidal-Volume Ventilation in The Acute Respiratory Distress SyndromeJimmy Christianto SuryoBelum ada peringkat
- Mechanical VentilationDokumen21 halamanMechanical VentilationWang EvanBelum ada peringkat
- PRESION Positiva HistoriaDokumen18 halamanPRESION Positiva HistoriaWALTER HUGO GOMEZBelum ada peringkat
- SMART Ventilation 101 2023Dokumen20 halamanSMART Ventilation 101 2023umar ankaBelum ada peringkat
- Mechanical VentilatorDokumen31 halamanMechanical VentilatorechtimBelum ada peringkat
- Overview of MechanicalDokumen16 halamanOverview of MechanicalRahul Deshmukh100% (1)
- Crit Care Nurse 2011 Grossbach 30 44Dokumen18 halamanCrit Care Nurse 2011 Grossbach 30 44Hanik FiriaBelum ada peringkat
- VENTILATOR PREPARATION and SETTINGDokumen22 halamanVENTILATOR PREPARATION and SETTINGArtha WigunaBelum ada peringkat
- Page 102-105 Positive Pressure VentilationDokumen3 halamanPage 102-105 Positive Pressure VentilationGrandisDekaBelum ada peringkat
- Machanical Ventilator Nursing Care PalnDokumen13 halamanMachanical Ventilator Nursing Care PalnAnnie Priscilla100% (1)
- Mechanical VentaDokumen84 halamanMechanical Ventaأبوأحمد الحكيم100% (1)
- Anesthesia For Tracheal Surgery - Specific Procedures - UpToDateDokumen29 halamanAnesthesia For Tracheal Surgery - Specific Procedures - UpToDateMaría Augusta Robayo UvilluzBelum ada peringkat
- Mechanical VentilationDokumen8 halamanMechanical VentilationMir MirBelum ada peringkat
- Modos Basicos de VentilacionDokumen16 halamanModos Basicos de Ventilacionbenitez1228Belum ada peringkat
- Westside Deli MenuDokumen6 halamanWestside Deli MenuCharlestonCityPaperBelum ada peringkat
- Plot Summary of Animal FarmDokumen1 halamanPlot Summary of Animal Farm10nov1964Belum ada peringkat
- 103 CÂU TỪ VỰNG TỪ ĐỀ CÔ VŨ MAI PHƯƠNGDokumen31 halaman103 CÂU TỪ VỰNG TỪ ĐỀ CÔ VŨ MAI PHƯƠNGDuong Hong AnhBelum ada peringkat
- Problems and SolutionsDokumen268 halamanProblems and SolutionsMajid Mohammadi100% (1)
- Case Report of Hernia Inguinalis Lateralis ReponibleDokumen23 halamanCase Report of Hernia Inguinalis Lateralis ReponibleMuhammad Ikhlas YasinBelum ada peringkat
- Abdomen - Pelvis: Lecturer: Prof. Dr. Wahyuni Lukita Atmodjo, PH.DDokumen33 halamanAbdomen - Pelvis: Lecturer: Prof. Dr. Wahyuni Lukita Atmodjo, PH.DAgatha FeliciaBelum ada peringkat
- Book of Horn and IvoryDokumen96 halamanBook of Horn and IvoryBen A.Belum ada peringkat
- Radiological Features of BronchiectasisDokumen24 halamanRadiological Features of BronchiectasisOxana TurcuBelum ada peringkat
- Doberman Pinscher: US TerminologyDokumen6 halamanDoberman Pinscher: US Terminologyclauba10100% (1)
- Animal FlashcardsDokumen31 halamanAnimal FlashcardsMary Grace PacianoBelum ada peringkat
- Wildlife Fact File - Birds - 11-20Dokumen20 halamanWildlife Fact File - Birds - 11-20ClearMind84Belum ada peringkat
- Ã'Tia' Fiakdkdhl Úohd, H - FLD U 07: D.S. Senanayake College - Colombo 07Dokumen12 halamanÃ'Tia' Fiakdkdhl Úohd, H - FLD U 07: D.S. Senanayake College - Colombo 07joker boyBelum ada peringkat
- The Wardrobe, The White Witch Has Magical Powers That Children Fear. She Can TurnDokumen3 halamanThe Wardrobe, The White Witch Has Magical Powers That Children Fear. She Can Turnxxbbb ddssBelum ada peringkat
- Belotero Product CatalogueDokumen36 halamanBelotero Product CatalogueNiculae Bogdan DimitrieBelum ada peringkat
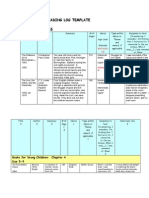
- Annotated Reading LogDokumen13 halamanAnnotated Reading LoggaureliBelum ada peringkat
- Ajara-Rasayana KSRPrasadDokumen56 halamanAjara-Rasayana KSRPrasadksr prasad100% (1)
- Blust 2000 - Origins DragonsDokumen19 halamanBlust 2000 - Origins DragonsFitri AmaliaBelum ada peringkat
- Cenozoic EraDokumen25 halamanCenozoic Erawinter padillaBelum ada peringkat
- Link To Publication in University of Groningen/UMCG Research DatabaseDokumen54 halamanLink To Publication in University of Groningen/UMCG Research DatabaseSrood TalibBelum ada peringkat
- Aspic TexturesDokumen3 halamanAspic TexturesRoy WinchesterBelum ada peringkat
- Ethical Issues in Conducting SIPDokumen60 halamanEthical Issues in Conducting SIPMavrichk100% (1)
- FoodDokumen54 halamanFoodBrihad Maurya0% (1)
- Grade 10 - Second Period - Set BookDokumen5 halamanGrade 10 - Second Period - Set BookMoh ArtkwBelum ada peringkat
- 6530-01-533-4863 - Table Surgical ISO - HANDBOOK - INSERT - STARTUPDokumen17 halaman6530-01-533-4863 - Table Surgical ISO - HANDBOOK - INSERT - STARTUPViniciusBelum ada peringkat
- Elicityl - OligoTech - Human Milk Oligosaccharides HMOs - 2011v2Dokumen4 halamanElicityl - OligoTech - Human Milk Oligosaccharides HMOs - 2011v2pascalsalvaBelum ada peringkat
- The Power of NetworkingDokumen12 halamanThe Power of Networkingapi-400197296Belum ada peringkat
- Arteries of AbdomenDokumen3 halamanArteries of Abdomenmero1983Belum ada peringkat
- Struktur Organisasi Puskesmas DoneDokumen19 halamanStruktur Organisasi Puskesmas Donepuskesmas kepulunganBelum ada peringkat
- ElectronicsDokumen41 halamanElectronicsKazelle BustamanteBelum ada peringkat
- THBT Animal Testing Should Be BannedDokumen3 halamanTHBT Animal Testing Should Be BannedFabio RizalBelum ada peringkat
- Arowana: The Complete Owner’s Guide for the Most Expensive Fish in the World - Arowana Fish Tank, Types, Care, Food, Habitat, Breeding, Mythology – Includes Silver, Platinum, Red, Jardini, Black, Golden, GreenDari EverandArowana: The Complete Owner’s Guide for the Most Expensive Fish in the World - Arowana Fish Tank, Types, Care, Food, Habitat, Breeding, Mythology – Includes Silver, Platinum, Red, Jardini, Black, Golden, GreenBelum ada peringkat
- The Big Book of Pet Names ~ More than 10,000 Pet Names! The Most Complete Guide to Pet Names & MeaningsDari EverandThe Big Book of Pet Names ~ More than 10,000 Pet Names! The Most Complete Guide to Pet Names & MeaningsBelum ada peringkat
- The Everything Aquarium Book: All You Need to Build the Acquarium of Your DreamsDari EverandThe Everything Aquarium Book: All You Need to Build the Acquarium of Your DreamsPenilaian: 5 dari 5 bintang5/5 (1)
- Freshwater Aquarium Models: Recipes for Creating Beautiful Aquariums That ThriveDari EverandFreshwater Aquarium Models: Recipes for Creating Beautiful Aquariums That ThrivePenilaian: 3.5 dari 5 bintang3.5/5 (4)
- The Dragon Behind the Glass: A True Story of Power, Obsession, and the World's Most Coveted FishDari EverandThe Dragon Behind the Glass: A True Story of Power, Obsession, and the World's Most Coveted FishPenilaian: 4 dari 5 bintang4/5 (62)
- Profitable Fish Farming From Scratch: Where To Begin, How To BeginDari EverandProfitable Fish Farming From Scratch: Where To Begin, How To BeginBelum ada peringkat
- Freshwater Aquariums: Basic Aquarium Setup and MaintenanceDari EverandFreshwater Aquariums: Basic Aquarium Setup and MaintenancePenilaian: 3 dari 5 bintang3/5 (1)
- Sharks: 101 Super Fun Facts And Amazing Pictures (Featuring The World's Top 10 Sharks With Coloring Pages)Dari EverandSharks: 101 Super Fun Facts And Amazing Pictures (Featuring The World's Top 10 Sharks With Coloring Pages)Penilaian: 3 dari 5 bintang3/5 (3)
- Biofloc Fish Farming for Dummies: The Beginner's Guide to Setting Up FarmDari EverandBiofloc Fish Farming for Dummies: The Beginner's Guide to Setting Up FarmBelum ada peringkat
- Livebearers: Understanding Guppies, Mollies, Swordtails and OthersDari EverandLivebearers: Understanding Guppies, Mollies, Swordtails and OthersBelum ada peringkat
- The Dragon Behind the Glass: A True Story of Power, Obsession, and the World's Most Coveted FishDari EverandThe Dragon Behind the Glass: A True Story of Power, Obsession, and the World's Most Coveted FishPenilaian: 4 dari 5 bintang4/5 (35)
- Sharks: 101 Super Fun Facts And Amazing Pictures (Featuring The World's Top 10 Sharks)Dari EverandSharks: 101 Super Fun Facts And Amazing Pictures (Featuring The World's Top 10 Sharks)Penilaian: 4 dari 5 bintang4/5 (8)
- Eye to Eye with Big Bass: “Let Her Go! She Is Just Another Big Fish!”Dari EverandEye to Eye with Big Bass: “Let Her Go! She Is Just Another Big Fish!”Belum ada peringkat
- Dolphins: 101 Fun Facts & Amazing Pictures (Featuring The World's 6 Top Dolphins)Dari EverandDolphins: 101 Fun Facts & Amazing Pictures (Featuring The World's 6 Top Dolphins)Penilaian: 4 dari 5 bintang4/5 (2)
- The Big Book Of Sea Monsters (Scary Looking Sea Animals): Animal Encyclopedia for KidsDari EverandThe Big Book Of Sea Monsters (Scary Looking Sea Animals): Animal Encyclopedia for KidsBelum ada peringkat
- Axolotl for beginners: 1x1 guide for species-appropriate keeping, care and feeding in the aquarium incl. interesting factsDari EverandAxolotl for beginners: 1x1 guide for species-appropriate keeping, care and feeding in the aquarium incl. interesting factsBelum ada peringkat
- 5th Grade Geography: Seas and Oceans of the World: Fifth Grade Books Marine Life and Oceanography for KidsDari Everand5th Grade Geography: Seas and Oceans of the World: Fifth Grade Books Marine Life and Oceanography for KidsBelum ada peringkat
- The New Saltwater Aquarium Guide: How to Care for and Keep Marine Fish and CoralsDari EverandThe New Saltwater Aquarium Guide: How to Care for and Keep Marine Fish and CoralsPenilaian: 5 dari 5 bintang5/5 (2)