Journal 2 PDF
Diunggah oleh
Jansenn DavidJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Journal 2 PDF
Diunggah oleh
Jansenn DavidHak Cipta:
Format Tersedia
Research Report
Physical Activity Promotion in the
Physical Therapy Setting: Perspectives
From Practitioners and Students
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
Debra Shirley, Hidde P. van der Ploeg, Adrian E. Bauman
D. Shirley, PT, PhD, FACP, is
Coordinator of Musculoskeletal
Background. Physical inactivity is a major risk factor for chronic disease. Primary Physiotherapy, Discipline of Phys-
health care practitioners are well placed to promote a physically active lifestyle. The iotherapy, Faculty of Health Sci-
perceptions and practice of physical therapists on their role in physical activity ences, University of Sydney, Syd-
promotion are not well known. ney, New South Wales, Australia.
H.P. van der Ploeg, PhD, is Senior
Objective. The objective of this study was to determine the knowledge, confi- Research Fellow, Cluster for Phys-
dence, role perception, barriers, feasibility, and counseling practice of physical ical Activity and Health, Sydney
therapists and physical therapist students regarding the promotion of nontreatment School of Public Health, University
of Sydney, Level 2, Medical Foun-
physical activity for better health.
dation Building (K25), Sydney,
New South Wales 2006, Australia.
Design. A cross-sectional survey was conducted. Address all correspondence to Dr
van der Ploeg at: hiddep@health.
Methods. In 2008, 321 (54%) of a random sample of all physical therapists usyd.edu.au.
registered in New South Wales, Australia, responded to a survey on their knowledge, A.E. Bauman, PhD, FAFPHM, is
confidence, role perception, barriers, feasibility, and counseling practice with regard Sesquicentenary Professor of Pub-
to promoting a physically active lifestyles to their patients. Physical therapist students lic Health (Behavioral Epidemiol-
(n⫽279) completed the same survey but without the questions on barriers and ogy and Health Promotion), Clus-
ter for Physical Activity and
counseling practice. Health, Sydney School of Public
Health, University of Sydney.
Results. Physical therapists and physical therapist students consider that it is part
[Shirley D, van der Ploeg HP, Bau-
of their role to give their patients nontreatment physical activity advice. Overall, they man AE. Physical activity promo-
reported having adequate knowledge and skills to undertake this role. Incorporating tion in the physical therapy
advice into normal consultations is deemed the most feasible form of lifestyle physical setting: perspectives from practi-
activity promotion in physical therapist practice. tioners and students. Phys Ther.
2010;90:1311–1322.]
Limitations. The cross-sectional nature of this study makes it difficult to deter- © 2010 American Physical Therapy
mine cause and effect relationships. Some selection bias may have occurred, as the Association
physical therapists who completed the questionnaires may have been those most
interested in physical activity promotion.
Conclusions. Physical therapist practice appears to be an excellent avenue for
promoting a physically active lifestyle and could potentially play an important public
health role.
Post a Rapid Response to
this article at:
ptjournal.apta.org
September 2010 Volume 90 Number 9 Physical Therapy f 1311
Physical Activity Promotion in Physical Therapy
P
hysical activity is accepted is an even more widespread public act in a primary prevention role. In
worldwide as a public health health problem, with only a quarter the United States, a survey of physi-
priority. A physically active life- of adults meeting the national phys- cal therapists indicated that increas-
style has been shown to significantly ical activity recommendations.7 The ing physical activity was the most
reduce the risk of developing cardio- public health challenge is to develop frequent area of focus for health pro-
vascular disease, obesity, type 2 dia- approaches that reach large numbers motion behavior.18 The physical
betes mellitus, several forms of can- of people with evidence-based pri- therapists’ confidence in prescribing
cer, and depression.1– 4 Regular mary prevention strategies. nontreatment physical activity pro-
physical activity decreases all-cause grams is the best predictor of
mortality risk by 20% to 30% com- Primary health care practitioners are whether physical activity is pre-
pared with insufficient activity.5 ideally positioned to promote physi- scribed.18 Although it is believed that
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
Most of these effects on all-cause cal activity as a health promotion physical therapists should be in-
mortality can be assigned to the pos- measure. Many patients in primary volved in physical activity promo-
itive effects of physical activity on care have health problems that could tion,17 the views of individual physi-
cardiovascular disease and cancer, be prevented by a physically active cal therapists about their potential
the leading causes of mortality and lifestyle.8 For the past decade, there role in physical activity promotion
morbidity in the Western world. has been a focus on using primary are not well known. Thus, the feasi-
care physicians to promote physical bility and acceptability of physical
This epidemiological evidence has activity. Strategies implemented by activity promotion in the physical
been synthesized into recommended primary care physicians have demon- therapy setting need to be ex-
levels of physical activity for meta- strated mixed success,9 –12 with most plored.19 The aim of this study was
bolic health and cardiovascular dis- programs showing modest effect to determine the knowledge, confi-
ease prevention by the American sizes and only in the short term.13 It dence, role perception, barriers, fea-
College of Sport Medicine and the has been suggested that a reasonable sibility, and counseling practice of
American Heart Association. The rec- approach for primary care physi- physical therapists and physical ther-
ommendation states that adults cians to adopt is to undertake brief apist students regarding the promo-
should be active 5 days per week and interventions with inactive patients tion of nontreatment physical activ-
have at least 30 minutes of moderate- who have health conditions that ity for better health.
intensity activity daily.1,3 Recom- could be reduced by physical activity
mended levels of physical activity for participation.13 However, the main Method
cardiovascular health can comprise barriers to health promotion identi- In June 2008, study survey question-
all types of regular activity, such as fied by primary care physicians are naires were mailed to a random sam-
structured exercise, active commut- perceived lack of training, beliefs ple of 602 physical therapists. This
ing, incidental activity and active liv- that they are unable to change health sample size was based on our earlier
ing, and active sports and recreation. habits, time constraints, and lack of work on primary care physicians,8
Only half of all Australian adults meet confidence.14,15 Although campaigns because no data were available for
these physical activity recommenda- about the importance of physical ac- physical therapists on the researched
tions,6 which means the other half is tivity have improved knowledge outcomes that would have justified
at increased risk of developing car- among primary care physicians, this a proper sample size calculation with-
diovascular disease, diabetes, obe- knowledge has not translated into out making ungrounded assumptions.
sity, several forms of cancer, and a counseling more patients in physical The random sample was drawn from
range of other chronic diseases. In activity.8,16 all physical therapists in New South
the United States, physical inactivity Wales, Australia, who were members
Physical therapists are primary care of the Australian Physiotherapy Asso-
practitioners who are thought to ciation. At the time of the survey,
have great potential for physical ac- there were 6,585 registered physical
Available With
This Article at tivity promotion.17 They prescribe therapists in New South Wales.20 To
ptjournal.apta.org exercise for a wide range of condi- maximize the response rate, the orig-
tions (mostly musculoskeletal) re- inal sample was sent a reminder to
• Audio Abstracts Podcast quiring rehabilitation. Currently, complete the survey questionnaire
physical therapy is mainly a tertiary if they had not returned it after 2
This article was published ahead of
print on July 22, 2010, at prevention discipline, even though months. Three different groups of
ptjournal.apta.org. physical therapists are equipped physical therapist students from the
with the ideal skills and potential to University of Sydney were surveyed
1312 f Physical Therapy Volume 90 Number 9 September 2010
Physical Activity Promotion in Physical Therapy
at the end of a lecture. First-year Table 1.
(n⫽161) and fourth-year (n⫽136) Personal Characteristics of the Physical Therapist Participants and of All Physical
students enrolled in the Bachelor of Therapists Registered in New South Wales, Australia
Applied Science in Physiotherapy All Physical
degree program and first-year stu- Therapists in New
Study Sample South Wales
dents (n⫽59) from the Masters of Variable (nⴝ319) (nⴝ6,585)20
Physiotherapy degree program were
Female, n (%) 233 (73) 4,863 (74)
invited to complete the survey. All
survey responses were entered by Age (y), n (%)
the same person into a preset data ⬍35 133 (42) 2,536 (38)
entry system, and approximately 10% 35–44 94 (29) 1,821 (28)
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
were randomly checked by one of 45–54 69 (22) 1,454 (22)
the other researchers for entry mis- ⱖ55 22 (7) 774 (12)
takes, which showed good data entry
Private practice, n (%) 182 (57) 3,753 (57)
quality.
Years in practice, mean (SD) 14 (11) NAa
Survey Design No. of patients treated per week, mean (SD) 50 (26) NA
The survey questionnaire was Hours worked per week, mean (SD) 34 (11) 33 (NA)
adapted from a previous survey ques- a
NA⫽not available.
tionnaire used in a study of primary
care physicians8 that was designed
based on focus groups with primary
care physicians and initial pilot test- determine relative proportions of ac- sons were made on knowledge, con-
ing.21 The adaptations made to the tive and inactive people.22 The phys- fidence, role perception, barriers,
questionnaire were minor and only ical therapist student survey was sim- feasibility, and counseling practice
aimed to make the questionnaire rel- ilar to the physical therapist survey of physical activity among groups us-
evant for physical therapists. The but did not include the items on ing multiple logistic regression anal-
survey questionnaire, presented in physical activity promotion practice yses. The logistic regression analyses
the Appendix, covered the following and barriers. were used to calculate odds ratios
topics: knowledge about the amount (ORs) to compare physical therapists
of physical activity required for Data Analysis who encouraged 10 or more patients
health benefits in adults (4 items), The responses to the questions on per month to become more active
perception of the role of physical knowledge, role perception, confi- with those who encouraged fewer
therapists in physical activity promo- dence, feasibility, and barriers were than 10 patients per month to be-
tion (2 items), confidence in promot- dichotomized by combining the 2 come more active. Similarly, ORs
ing physical activity (3 items), barri- “agree” options and combining the were calculated using logistic regres-
ers to physical activity promotion (6 “neutral” with the 2 “disagree” op- sion to compare the physical thera-
items), and feasibility of different tions. The question on numbers of pists, the fourth-year bachelor’s de-
physical activity promotion strate- patients counseled about physical gree students, and the first-year
gies (4 items). All items were scored activity each month was dichoto- master’s degree students with the
on a 5-point Likert scale. Physical mized at 10 or more per month and first-year bachelor’s degree students.
therapists also were asked about the fewer than 10 per month, because All logistic regression analyses were
number of patients they had encour- this division resulted in 2 groups of checked for possible confounding
aged in the previous month to lead a almost equal size and thus optimized among groups from participants’
more physically active lifestyle. Fi- statistical power for the analysis. sex, years in practice, hours worked
nally, general demographic data per week, and number of patients
were recorded, and participants Descriptive analysis was used to pro- treated per week. Possible con-
were asked how they would rate vide a basic quantitative description founders were added to the regres-
their own physical activity levels of the data set. The personal charac- sion model; variables that changed
compared with those of other Aus- teristics of all physical therapists reg- the OR by at least 10% were identi-
tralians of the same sex and age on a istered in New South Wales were re- fied as confounders and were cor-
5-point scale (ranging from “much ported to give an indication of how rected for in the final analysis. The
more active” to “much less active”), representative our physical therapist logistic regression analyses were re-
which has been shown to reliably sample was.20 Inferential compari- peated to stratify for physical thera-
September 2010 Volume 90 Number 9 Physical Therapy f 1313
Physical Activity Promotion in Physical Therapy
pists working in the public and pri- tivity advice more frequently and P⬍.01) as feasible avenues for phys-
vate health care sectors. All analyses those who gave less advice with re- ical activity promotion, whereas
were performed in SPSS version 17.* gard to their knowledge of the phys- group sessions were thought to be
ical activity message. However, only less suitable (OR⫽0.55, P⫽.01).
Role of the Funding Source one third of the respondents could
The project was financed through an name the national physical activity Table 3 shows the results of the com-
Australian Government National recommendation for Australian parison of physical therapist stu-
Health and Medical Research Coun- adults. In both groups, almost all dents and practicing physical thera-
cil program grant (#301200) held by physical therapists thought it should pists with regard to knowledge, role
Dr Bauman. be part of their role to give their perception, confidence, and feasibil-
patients physical activity advice. ity of physical activity promotion.
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
Results Physical therapists who gave more Knowledge of the public health
A total of 319 physical therapists patients physical activity advice physical activity message showed a
(54%) and 279 (78%) students com- were more likely to feel confident in gradual improvement from the first-
pleted the survey. The personal char- suggesting specific physical activity year bachelor’s degree students on-
acteristics of the participating phys- programs. They also were less likely ward. Almost all respondents agreed
ical therapists are described in Table to identify lack of time or the per- that promoting a physically active
1, which also describes the personal ception that it would not change the lifestyle is part of the role of a phys-
characteristics of all physical thera- patient’s behavior as barriers to pro- ical therapist, and as students
pists registered in New South Wales. moting a physically active lifestyle in progress toward being graduate
The proportion of female respon- their patients. Overall, physical ther- physical therapists, their confidence
dents was greater in the physical apists generally did not identify in promoting physical activity
therapist group (73%) compared many barriers to promoting physical grows. The most feasible method of
with the student groups, which had activity to their patients. Almost all promoting physical activity seems to
a more even distribution of female to physical therapists thought it would be incorporating brief counseling
male respondents (58% female year 1 be feasible to incorporate brief phys- into a normal consultation, with pro-
bachelor’s degree students, 68% fe- ical activity counseling into regular vision of resources as the next most
male year 4 bachelor’s degree stu- treatment sessions. Separate one-on- feasible method.
dents, and 52% female master’s de- one and group physical activity con-
gree students). The majority of sultations were thought to be less Discussion
physical therapists and students con- feasible, although almost two thirds The current study indicates that
sidered themselves more physically of the physical therapists who gave physical therapists and physical ther-
active than other Australians of their physical activity advice more fre- apist students believe that physical
same sex and age (Tabs. 2 and 3). quently still thought these were fea- activity prescription for health pro-
sible avenues for physical activity motion should be part of their role
More than half of the physical thera- promotion. Ninety percent of physi- and that they would be confident in
pists (54%) reported that they en- cal therapists also thought it would this role. Integrating brief counseling
couraged 10 or more patients each be feasible to distribute physical ac- into usual treatment sessions was
month to lead a more physically ac- tivity promotion resources. thought to be the most feasible form
tive lifestyle (beyond therapeutic ex- of physical activity promotion in
ercises). Table 2 presents the knowl- Physical therapists working in the physical therapist practice, followed
edge, role perception, confidence, public and private health care sec- by the distribution of resources such
barriers, and feasibility of physical tors showed similar responses to the as brochures.
activity promotion for physical ther- survey (data not shown). However,
apists who encouraged 10 or more physical therapists in private prac- The results of our study are compa-
patients per month to become more tice were less likely to report that rable to the attitudes of Australian
active and those who encouraged physical activity promotion would primary care physicians who com-
fewer than 10 patients per month to not change the patients’ behavior pleted a similar survey that indicated
become more active. There were no (OR⫽0.38, P⬍.01). Compared with 98% believed physical activity pro-
major differences between the phys- the public sector, private practice motion was part of the physician’s
ical therapists who gave physical ac- physical therapists more frequently role.16 However, the surveyed physi-
identified usual treatment consulta- cians felt less confident in giving
* SPSS Inc, 233 S Wacker Dr, Chicago, IL tions (OR⫽3.76, P⬍.01) or separate physical activity advice than the cur-
60606. one-on-one sessions (OR⫽1.99, rent sample of physical therapists,
1314 f Physical Therapy Volume 90 Number 9 September 2010
Physical Activity Promotion in Physical Therapy
Table 2.
Physical Therapists’ Knowledge, Role Perception, Confidence, Barriers, and Feasibility of Physical Activity Promotiona
Odds Ratio (95% CI) for
Counseled <10 Counseled >10 Physical Therapists Who
Patients/Month Patients/Month Counseled >10 Patients/Month
Variable (nⴝ140), n Agree (%) (nⴝ165), n Agree (%) Compared With <10b
Knowledge of PA message
Taking the stairs at work and generally being 80 (58) 83 (51) 0.70 (0.44–1.13)
more active each day is enough PA to
improve health
Half an hour of walking on most days is all the 77 (56) 100 (61) 1.40 (0.87–2.26)
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
exercise that is needed for good health
Exercise that is good for health must make you 35 (25) 45 (27) 1.12 (0.66–1.91)
puff and pant
Several short walks of 10 minutes each on 99 (71) 132 (80) 1.83 (1.05–3.17)c
most days is better than one round of golf
per week for good health
Physical therapist’s role
Discussing the benefits of a physically active 132 (94) 160 (97) 1.69 (0.53–5.39)
lifestyle with patients is part of the physical
therapist’s role
Suggesting to patients ways to increase daily 130 (93) 161 (98) 3.07 (0.92–10.25)
PA is part of the physical therapist’s role
Physical therapists should be physically active 127 (91) 158 (96) 2.58 (0.97–6.85)
to act as a role model for their patients
Confidence in giving PA message
I would feel confident in giving general advice 134 (96) 160 (97) 1.28 (0.37–4.38)
to patients on a physically active lifestyle
I would feel confident in suggesting specific PA 121 (87) 156 (96) 2.48 (1.03–5.99)c
programs for my patients
Barriers to PA promotion
Lack of time 47 (34) 25 (15) 0.32 (0.18–0.57)c
Lack of counseling skills 11 (8) 0 (0)
Lack of remuneration for promoting PA 12 (9) 15 (9) 0.85 (0.37–1.96)
Lack of interest in promoting PA 2 (1) 1 (1)
Feeling it would not change the patient’s 28 (20) 9 (6) 0.25 (0.11–0.56)c
behavior
Feeling it would not be beneficial for the 3 (2) 1 (1)
patient
Feasibility of PA promotion strategies
Brief counseling integrated into regular 122 (88) 158 (97) 3.65 (1.29–10.31)c
consultations
Separate one-on-one consultations 46 (33) 102 (63) 3.25 (1.98–5.32)c
Group sessions 67 (48) 98 (60) 1.69 (1.05–2.72)c
Distribution of resources (eg, brochures) 124 (89) 147 (90) 1.14 (0.53–2.45)
Physical therapist’s PA level
How physically active do you think you are 103 (74) 137 (83) 1.67 (0.94–2.98)
currently compared with other Australians of
your sex and age? (agree⫽more active)
Are you aware of the physical activity 46 (35) 56 (34) 1.09 (0.66–1.79)
guidelines
a
CI⫽confidence interval, PA⫽physical activity.
b
Adjusted for participants’ sex and years in physical therapist practice.
c
P⬍.05.
September 2010 Volume 90 Number 9 Physical Therapy f 1315
Physical Activity Promotion in Physical Therapy
Table 3.
Comparison of Physical Therapist Students and Practicing Physical Therapists With Regard to Knowledge, Role Perception,
Confidence, and Feasibility of Physical Activity Promotiona
Group (Students or n Agree Odds Ratio
Variable Physical Therapists) (%) (95% CI)b
Knowledge of PA message
Taking the stairs at work and generally being more active each day is enough PA BSc, year 1c 33 (36) 1.00
to improve health BSc, year 4d 48 (38) 1.10 (0.63–1.93)
MP, year 1e 22 (44) 1.38 (0.71–2.70)
PTf 167 (53) 1.95 (1.20–3.16)g
Half an hour of walking on most days is all the exercise that is needed for good BSc, year 1 26 (28) 1.00
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
health BSc, year 4 48 (38) 1.53 (0.86–2.75)
MP, year 1 29 (48) 2.48 (1.25–4.92)g
PT 187 (59) 3.64 (2.08–5.77)g
Exercise that is good for health must make you puff and pant BSc, year 1 31 (34) 1.00
BSc, year 4 35 (28) 0.82 (0.45–1.47)
MP, year 1 22 (37) 1.14 (0.57–2.26)
PT 85 (27) 0.77 (0.47–1.27)
Several short walks of 10 minutes each on most days is better than one round of BSc, year 1 57 (63) 1.00
golf per week for good health BSc, year 4 86 (69) 1.28 (0.73–2.27)
MP, year 1 41 (67) 1.19 (0.60–2.37)
PT 244 (77) 1.96 (1.19–3.24)g
Physical therapist’s role
Discussing the benefits of a physically active lifestyle with patients is part of the BSc, year 1 84 (91) 1.00
physical therapist’s role BSc, year 4 119 (94) 1.61 (0.56–4.63)
MP, year 1 57 (93) 1.80 (0.46–7.07)
PT 305 (96) 2.11 (0.85–5.24)
Suggesting to patients ways to increase daily PA is part of the physical therapist’s BSc, year 1 75 (82) 1.00
role BSc, year 4 119 (94) 3.61 (1.42–9.23)g
MP, year 1 55 (90) 2.33 (0.80–6.74)
PT 305 (96) 4.73 (2.19–10.19)g
Physical therapists should be physically active to act as a role model for their BSc, year 1 88 (96) 1.00
patients BSc, year 4 115 (91) 0.46 (0.14–1.51)
MP, year 1 52 (85) 0.26 (0.08–0.88)g
PT 298 (93) 0.63 (0.21–1.91)
I would encourage most my patients to have a physically active lifestyle if I were BSc, year 1 89 (97) 1.00
in physical therapist practice BSc, year 4 116 (92) 0.50 (0.05–4.95)
MP year 1 60 (98) 2.19 (0.02–1.56)
PT NA NA
Confidence in giving PA message
I would feel confident in giving general advice to patients on a physically active BSc, year 1 80 (87) 1.00
lifestyle BSc, year 4 110 (87) 1.16 (0.51–2.64)
MP, year 1 58 (95) 4.23 (0.91–19.69)
PT 308 (97) 4.64 (1.95–11.01)g
I would feel confident in suggesting specific PA programs for my patients BSc, year 1 62 (67) 1.00
BSc, year 4 102 (81) 2.28 (1.20–4.30)g
MP, year 1 57 (93) 9.09 (2.62–31.51)g
PT 290 (91) 5.54 (3.05–10.06)g
(Continued)
with about 22% fewer physicians physical therapists identified few sive training in exercise prescription
feeling confident in giving specific barriers to promoting an active life- for treatment purposes and at present
physical activity advice.16 This find- style, whereas a number of those same mainly operate in a tertiary prevention
ing gives physical therapists an ad- barriers are known to frequently pre- capacity. Our results support the ear-
vantage over other primary care vent physicians from promoting phys- lier notion that physical therapists are
practitioners in successfully integrat- ical activity, especially lack of time, underutilized for promoting a physi-
ing lifestyle physical activity promo- absence of reimbursements, and lim- cally active lifestyle and appear to be
tion into practice. Furthermore, our ited counseling skills.8,23,24 In con- well placed to play an important pub-
findings showed that the surveyed trast, physical therapists have exten- lic health role.17,25
1316 f Physical Therapy Volume 90 Number 9 September 2010
Physical Activity Promotion in Physical Therapy
Table 3.
Continued
Group (Students or n Agree Odds Ratio
Variable Physical Therapists) (%) (95% CI)b
Feasibility of PA promotion strategies
Brief counseling integrated into regular consultations BSc, year 1 59 (65) 1.00
BSc, year 4 92 (73) 1.60 (0.88–2.89)
MP, year 1 53 (87) 3.48 (1.47–8.24)g
PT 293 (93) 7.15 (3.88–13.17)g
Separate one-on-one consultations BSc, year 1 50 (55) 1.00
BSc, year 4 55 (44) 0.65 (0.37–1.12)
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
MP, year 1 19 (31) 0.35 (0.17–0.69)g
PT 157 (50) 0.83 (0.52–1.34)
Group sessions BSc, year 1 60 (66) 1.00
BSc, year 4 105 (83) 2.72 (1.43–5.20)g
MP, year 1 36 (59) 0.72 (0.37–1.41)
PT 174 (55) 0.65 (0.40–1.05)
Distribution of resources (such as brochures) BSc, year 1 62 (68) 1.00
BSc, year 4 108 (86) 2.74 (1.41–5.35)g
MP, year 1 49 (80) 2.09 (0.95–4.60)
PT 282 (89) 3.84 (2.17–6.80)g
PA level
How physically active do you think you are currently compared with other BSc, year 1 55 (60) 1.00
Australians of your sex and age? (agree⫽more active) BSc, year 4 66 (53) 0.81 (0.46–1.41)
MP, year 1 43 (71) 1.47 (0.73–2.98)
PT 248 (77) 2.59 (1.56–4.30)g
a
CI⫽confidence interval, PA⫽physical activity, BSc⫽Bachelor of Applied Science in Physiotherapy degree program, MP⫽Master of Physiotherapy degree
program, PT⫽physical therapist.
b
Adjusted for participants’ sex.
c
n⫽92 in BSc program, year 1 (⫽reference category).
d
n⫽127 in BSc program, year 4.
e
n⫽59 in MP program, year 1.
f
n⫽319 of the surveyed physical therapists.
g
P⬍.05.
Although the role of physical thera- pressure, although it was not clear Physical therapists who already gave
pists as promoters of a physically ac- how frequently physical therapists more patients physical activity life-
tive lifestyle has received only lim- prescribed physical activity for con- style advice also appeared to have
ited attention in the literature, this ditions other than musculoskeletal somewhat greater knowledge about
role is believed to be appropriate for conditions. People receiving physi- physical activity promotion. This re-
these primary care practitioners.18,25,26 cal activity lifestyle advice in a phys- sult is similar to that for physicians;
In 3 US states, when physical thera- ical therapy outpatient department those who attended relevant work-
pists’ perceptions of health promo- in Australia were more likely to in- shops were more likely to give phys-
tion behaviors were surveyed, it was crease their average weekly physical ical activity advice.8 Physical thera-
apparent that 54% believed physical activity by 60 minutes compared pists who gave more patients
therapists were involved in promo- with a control group.25 However, physical activity advice also were
tion of health and fitness.18 In Swe- this was the only significant differ- slightly more confident and reported
den, an audit of the amount of phys- ence evident between the groups in fewer barriers to promoting physical
ical activity prescription by various the average weekly physical activity activity in their practice. Because of
health care professionals indicated measures in this controlled inter- the cross-sectional nature of our
that physical therapists provided the vention trial. The authors stated that study, cause and effect are difficult
highest number of physical activity the capacity of physical therapists to to determine. Thus, it remains un-
referrals, with physicians providing promote physical activity for non- clear whether the physical thera-
the lowest.26 The most common rea- therapeutic purposes could be fur- pists’ better knowledge and confi-
sons for physical activity prescription ther improved, but that the physical dence and lower perceived barriers
were musculoskeletal conditions, therapy setting was a feasible avenue enabled them to integrate physical
obesity, diabetes, and high blood for promoting an active lifestyle. activity promotion more easily into
September 2010 Volume 90 Number 9 Physical Therapy f 1317
Physical Activity Promotion in Physical Therapy
their daily practice, or whether these Comparison among the groups of responded to the survey. Physical
factors improved because they had students revealed some interesting therapists who chose to participate
already incorporated physical activity differences that may be accounted may have been those who are more
promotion more into their routine for by their different backgrounds, as interested in physical activity and
care. Physical therapists’ awareness well as their increasing knowledge health promotion in general. Thus,
of the physical activity guidelines acquired through their studies. The our results might have overestimated
was not correlated with the number bachelor’s degree students were pri- the perceived role, confidence, and
of patients counseled, on average, marily high school graduates en- feasibility of promoting a physically
and was surprisingly low, with just rolled in their first degree program, active lifestyle in physical therapist
one third aware of the national phys- whereas the master’s degree stu- practice. However, comparison of
ical activity guidelines. dents all had a bachelor’s degree in a the personal characteristics of our
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
major such as exercise and sport sci- sample with those of all physical
Physical therapists indicated that ences or human movement science. therapists registered in New South
separate, one-on-one consultations Many of the master’s degree students Wales (Tab. 1) suggests that our
are less feasible for physical activity had held jobs in gymnasium environ- study sample was representative for
promotion, and incorporating non- ments or as personal trainers, where the physical therapy workforce in
treatment physical activity advice their primary role was to assist peo- New South Wales for at least these
into normal consultations is deemed ple with exercise training. Our re- personal characteristics. Finally, the
feasible by almost all physical thera- sults showed that the further the stu- study sample size might have been
pists. Previous intervention work in dents had advanced through their insufficient to detect significant dif-
the rehabilitation setting has shown studies, the more likely they were to ferences among groups for some of
that a physical activity counselor can have perceptions similar to those of the variables that were studied.
effectively improve patients’ daily the practicing physical therapists.
physical activity levels in a series of Conclusion
one-on-one counseling sessions.27,28 This finding suggests that the stu- This study highlights the previously
In light of our findings, integrating a dents were learning about the possi- untapped potential for physical ther-
similar intervention into physical bilities of promoting nontreatment apists to give nontreatment physical
therapist practice might be feasible if physical activity through physical activity advice during regular treat-
the physical therapist would give a therapist practice during their cur- ment. Physical therapists, current
brief physical activity promotion in- rent physical therapy curriculum. and future, recognize this as one of
tervention during or following the However, it also has been suggested their roles and are confident in their
treatment sessions that the patients that the capacity of Australian phys- ability to promote lifestyle physical
receive for their initial health condi- ical therapists to give their patients activity. They perceive few barriers
tion. This strategy would use the physical activity advice for nontreat- to promoting physical activity and
physical therapist’s knowledge and ment purposes could be improved believe that integrating brief coun-
skills in exercise prescription, while further and could possibly be better seling into usual treatment sessions
simplifying the logistics of the inter- embedded in the physical therapy is the most feasible form of physical
vention and making the intervention curriculum.25 Furthermore, the cur- activity promotion in physical thera-
more convenient for the patient. rent study only surveyed students pist practice. The results of this
Such an intervention strategy also from one university, so it is possible study highlight the need to further
would lower the costs, as the physi- that students from universities with explore the possibilities to integrate
cal activity advice would be built somewhat different curricula would lifestyle physical activity promotion
into existing consultation time for have answered these questions into physical therapist practice to de-
another condition, and would make differently. termine its potential important role
good use of clinical contact time, as in public health.
well as build on the patient-therapist The main limitations of this study are
relationship. As treatment by a phys- the cross-sectional nature of the All authors provided concept/idea/research
ical therapist usually is spread out over study and the potential selection bias design, writing, and consultation (including
several sessions over a number of of study recruitment. Although our review of manuscript before submission). Dr
weeks, this duration will allow time survey had a higher response rate Shirley and Dr van der Ploeg provided data
collection and analysis. Dr van der Ploeg and
for the provision of sequential physical (54%) than a similar survey of pri-
Dr Bauman provided project management.
activity advice that has previously mary care physicians (40%),16 only Dr Shirley provided participants. Dr Bauman
been shown to be important for effec- just over half of the invited, ran- provided facilities/equipment and institu-
tive physical activity promotion.27,28 domly sampled physical therapists tional liaisons. The authors thank the Austra-
1318 f Physical Therapy Volume 90 Number 9 September 2010
Physical Activity Promotion in Physical Therapy
lian Physiotherapy Association for help with 8 van der Ploeg HP, Smith BJ, Stubbs T, et al. 19 Harris P, Smith BJ. Beliefs, Attitudes and
the distribution of the study survey Physical activity promotion: Are GPs get- Practices Among GPs in Relation to the
ting the message? Aust Fam Physician. Promotion of Physical Activity in Gen-
questionnaires. 2007;36:871– 874. eral Practice: A Qualitative Study. Report
CPAH 03– 0003. Melbourne, Australia: The
The study was approved by the Human Re- 9 Eaton CB, Menard LM. A systematic review National Institute of Clinical Studies; 2003.
search Ethics Committee of the University of of physical activity promotion in primary
care office settings. Br J Sports Med. 1998; 20 Profile of the Physiotherapists Workforce
Sydney. 32:11–16. in NSW. Sydney, Australia: New South
Wales Department of Health; 2009.
The project was financed through an Austra- 10 Hillsdon M, Thorogood M, White I, Foster
lian Government National Health and Med- C. Advising people to take more exercise 21 Mark A, Miners A, Bauman, Wallner F. Il-
is ineffective: a randomized controlled lawarra Physical Activity Project. Wol-
ical Research Council program grant trial of physical activity promotion in pri- longong, Australia: University of Wollon-
(#301200) held by Dr Bauman. mary care. Int J Epidemiol. 2002;31:808 – gong; 1999.
815.
This article was submitted November 16, 22 Slater CH, Green LW, Vernon SW, Keith
11 Lawlor DA, Hanratty B. The effect of phys-
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
VM. Problems in estimating the preva-
2009, and was accepted May 15, 2010. ical activity advice given in routine pri- lence of physical activity from national sur-
mary care consultations: a systematic re- veys. Prev Med. 1987;16:107–118.
DOI: 10.2522/ptj.20090383 view. J Public Health Med. 2001;23:219 – 23 Bull FC, Schipper EC, Jamrozik K,
226. Blanksby BA. Beliefs and behaviour of gen-
12 Marshall AL. Booth ML. Bauman AE. Pro- eral practitioners regarding promotion of
References moting physical activity in Australian gen- physical activity. Aust J Public Health.
1 Bauman AE. Updating the evidence that eral practices: a randomised trial of health 1995;19:300 –304.
physical activity is good for health: an ep- promotion advice versus hypertension
idemiological review 2000 –2003. J Sci 24 Eakin EG, Smith BJ, Bauman AE. Evaluating
management. Patient Educ Couns. 2005;
Med Sport. 2004;7(suppl 1):6 –19. the population health impact of physical
56:283–290. activity interventions in primary care: are
2 Garrett NA, Brasure M, Schmitz KH, et al. 13 Smith BJ, Merom D, Harris P, Bauman AE. we asking the right questions? J Phys Ac-
Physical inactivity: direct cost to a health Do Primary Care Interventions to Pro- tivity Health. 2005;2:197–215.
plan. Am J Prev Med. 2004;27:304 –309. mote Physical Activity Work? Report 25 Sheedy J, Smith B, Bauman A, et al. A con-
3 Haskell WL, Lee I, Pate RR, et al. Physical CPAH 03– 0002. Melbourne, Australia: Na- trolled trial of behavioural education to
activity and public health: updated recom- tional Institute of Clinical Studies; 2002. promote exercise among physiotherapy
mendations for adults from the American 14 Bauman A, Mant A, Middleton, et al. Do outpatients. Aust J Physiother. 2000;46:
College of Sport Medicine and the Ameri- general practitioners promote health? A 281–289.
can Heart Association. Med Sci Sports Ex- needs assessment. Med J Aust. 1989;151:
erc. 2007;39:1423–1434. 26 Leijon ME, Bendtsen P, Nilsen P, et al.
262–269. Physical activity referrals in Swedish pri-
4 Mathers CD, Vos ET, Stevenson CE, Begg 15 Pinto BM, Goldstein MG, Marcus BH. Ac- mary care: prescriber and patient charac-
SJ. The Australian Burden of Disease Study: tivity counseling by primary care physi- teristics, reasons for prescriptions, and
measuring the loss of health from diseases, cians. Prev Med. 1998;27:506 –513. prescribed activities. BMC Health Serv
injuries and risk factors. Med J Aust. 2000; Res. 2008;8:201.
172:592–596. 16 Buffart LM, van der Ploeg HP, Smith BJ,
et al. General practitioners’ perceptions 27 van der Ploeg HP, Streppel KR, Van der
5 Lee IM, Skerrett PJ. Physical activity and and practice of physical activity counsel- Beek AJ, et al. Counselling increases phys-
all-cause mortality: what is the dose- ling: changes over the past 10 years. Br J ical activity behaviour nine weeks after
response relation? Med Sci Sports Exerc. Sports Med. 2009;43:1149 –1153. rehabilitation. Br J Sports Med. 2006;40:
2001;33(suppl 6):S459 –S471. 223–229.
17 Verhagen E, Engbers L. The physical ther-
6 Chau J, Smith BJ, Bauman A, et al. Recent apist’s role in physical activity promotion. 28 van der Ploeg HP, Streppel KR, Van der
trends in physical activity in New South Br J Sports Med. 2009;43:99 –101. Beek AJ, et al. Successfully increasing
Wales. Is the tide of inactivity turning? physical activity behaviour after rehabilita-
Aust N Z J Public Health. 2008;32:82– 85. 18 Rea BL, Hopp Marshak H, Neish C, Davis tion. Am J Health Promot. 2007;
N. The role of health promotion in physi-
7 Brownson RC, Boehmer TK, Luke DA. De- 21:153–159.
cal therapy in California, New York, and
clining rates of physical activity in the Tennessee. Phys Ther. 2004;84:510 –523.
United States: what are the contributors?
Annu Rev Public Health. 2005;26:421– 443.
September 2010 Volume 90 Number 9 Physical Therapy f 1319
Physical Activity Promotion in Physical Therapy
Appendix.
Questionnaire for Physical Therapistsa
Physical Activity in Physical Therapist Practice
Physical Activity: includes any activity from a low intensity level, such as walking, to a high intensity level, such as
playing a competitive sport.
1. How often did you encourage your patients to have a more physically active lifestyle (beyond therapeutic exercise)
in the last month? (please tick one)
E Never E Often, perhaps 6 –9 patients
E Rarely, only 1 or 2 patients E More often, 10 or more patients
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
E Sometimes, perhaps 3–5 patients
2. To what extent do you agree or disagree with the following statements: (circle only one for each statement)
Strongly Not Strongly
Agree Agree Sure Disagree Disagree
a. Taking the stairs at work and generally 1 2 3 4 5
being more active each day is enough
physical activity to improve health
b. Half an hour of walking on most days 1 2 3 4 5
is all the exercise that is needed for
good health
c. Exercise that is good for health must 1 2 3 4 5
make you puff and pant
d. Several short walks of 10 minutes each 1 2 3 4 5
on most days is better than one round
of golf per week for good health
e. Discussing the benefits of a physically 1 2 3 4 5
active lifestyle with patients is part of
the physical therapist’s role
f. Suggesting to patients ways to 1 2 3 4 5
increase daily physical activity is
part of the physical therapist’s role
g. I feel confident in giving general 1 2 3 4 5
advice to patients on a physically
active lifestyle
h. I feel confident in suggesting specific 1 2 3 4 5
physical activity programs for my
patients
i. Physical therapists should be physically 1 2 3 4 5
active to act as a role model for their
patients
(Continued)
1320 f Physical Therapy Volume 90 Number 9 September 2010
Physical Activity Promotion in Physical Therapy
Appendix.
Continued
3. How often does the following prevent you from promoting a physically active lifestyle in your patients (beyond
therapeutic exercise)? (circle only one for each statement)
Very
Never Rarely Sometimes Often Often
a. Lack of time 1 2 3 4 5
b. Lack of counseling skills 1 2 3 4 5
c. Lack of remuneration for 1 2 3 4 5
promoting physical activity
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
d. Lack of interest in 1 2 3 4 5
promoting physical activity
e. Feeling it would not change 1 2 3 4 5
the patient’s behavior
f. Feeling it would not be 1 2 3 4 5
beneficial for the patient
g. Other:______________ 1 2 3 4 5
4. What kinds of physical activity promotion (beyond therapeutic exercise) would be feasible for you to deliver to
your patients? (circle only one for each statement)
Not
Highly Somewhat Not Really Totally
Feasible Feasible Sure Feasible Unfeasible
a. Brief counseling integrated 1 2 3 4 5
into your regular consultations
b. Separate one-on-one consultations 1 2 3 4 5
c. Group sessions 1 2 3 4 5
d. Distribution of resources 1 2 3 4 5
(eg, brochures)
5. Some general questions about your practice:
a. Average number of patients _________
you see each week:
b. Your number of years in _________
practice:
c. Your sex: E Female E Male
d. Your age in years: E ⬍35 E 35– 44 E 45–54 E ⬎54
e. Usual number of hours _________
worked each week:
f. The postal code where you _________
work:
g. In what area of physical E Musculoskeletal E Cardiopulmonary
therapy do you practice? E Neurological E Pediatrics
(please tick as many as are E Geriatrics E Occupational health and safety
applicable)
h. In what kind of practice do E Private practice
you work? E Community
E Public hospital (Continued)
September 2010 Volume 90 Number 9 Physical Therapy f 1321
Physical Activity Promotion in Physical Therapy
Appendix.
Continued
6. a. Are you aware of the National Physical Activity E E
Recommendation for Australian Adults? Yes No
b. If yes, please describe the National Physical Activity Recommendation for Australian Adults here.
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Downloaded from https://academic.oup.com/ptj/article-abstract/90/9/1311/2738092 by guest on 26 July 2019
7. Finally, about your own physical activity: How physically active do you think you are currently compared with
other Australians of your sex and age? (please tick one)
E Much more active E Slightly more active E About the same E Slightly less active E Much less active
a
The questionnaire may not be used or reproduced without written permission from the authors, except when referenced appropriately for noncommercial
scientific purposes.
1322 f Physical Therapy Volume 90 Number 9 September 2010
Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Case Study Research - Design and Methods, Third Edition, Applied Social Research Methods Series, Vol 5 (PDFDrive)Dokumen365 halamanCase Study Research - Design and Methods, Third Edition, Applied Social Research Methods Series, Vol 5 (PDFDrive)Rafid Chy86% (7)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Tutorial Interpolation in QGISDokumen3 halamanTutorial Interpolation in QGISMarcos José Falcão De Medeiros FilhoBelum ada peringkat
- F&B Waste Management QuestionnaireDokumen3 halamanF&B Waste Management QuestionnairePranav Kakà Harmilapi70% (27)
- Practical Research 2 Module 3Dokumen11 halamanPractical Research 2 Module 3Angela Rae90% (10)
- PE ABH What Is A Stress Test UCM - 300453 PDFDokumen2 halamanPE ABH What Is A Stress Test UCM - 300453 PDFJansenn DavidBelum ada peringkat
- PDF Download Ther Ex Notes Clinical Pocket Guide Daviss NotesDokumen2 halamanPDF Download Ther Ex Notes Clinical Pocket Guide Daviss NotesJansenn David0% (1)
- Physiotherapy Guideline COVID-19 FINAL PDFDokumen28 halamanPhysiotherapy Guideline COVID-19 FINAL PDFJansenn DavidBelum ada peringkat
- 5 Things To Know HDokumen1 halaman5 Things To Know HJansenn DavidBelum ada peringkat
- Physiotherapy Guideline COVID-19 FINAL PDFDokumen28 halamanPhysiotherapy Guideline COVID-19 FINAL PDFJansenn DavidBelum ada peringkat
- Sample Chapter 8 Therapeutic ExerciseDokumen29 halamanSample Chapter 8 Therapeutic ExerciseAnsh TanwarBelum ada peringkat
- Admas University: Migrating To New Technology Individual AssignmentDokumen11 halamanAdmas University: Migrating To New Technology Individual AssignmentephaBelum ada peringkat
- Designing A Strategic Information Systems Planning Methodology For Malaysian Institutes of Higher Learning (Isp-Ipta)Dokumen8 halamanDesigning A Strategic Information Systems Planning Methodology For Malaysian Institutes of Higher Learning (Isp-Ipta)Janet G.Belum ada peringkat
- Thematic Analysis: Dr. Rania AlbsoulDokumen31 halamanThematic Analysis: Dr. Rania AlbsoulAhmad AltarefeBelum ada peringkat
- Climate Change Strategies' Model in Teaching Science 7Dokumen10 halamanClimate Change Strategies' Model in Teaching Science 7Psychology and Education: A Multidisciplinary JournalBelum ada peringkat
- Backward Elimination and Stepwise RegressionDokumen5 halamanBackward Elimination and Stepwise RegressionNajwa AmellalBelum ada peringkat
- Legal Translation and Bilingual Law Drafting in Hong Kong - Challenges and Interactions in Chinese RegionsDokumen172 halamanLegal Translation and Bilingual Law Drafting in Hong Kong - Challenges and Interactions in Chinese RegionsPui Gwen YeungBelum ada peringkat
- MCA - Tier II - SARDokumen44 halamanMCA - Tier II - SARGirish JadhavBelum ada peringkat
- SIP Report FormatDokumen11 halamanSIP Report Formatsanjeetmohanty9884Belum ada peringkat
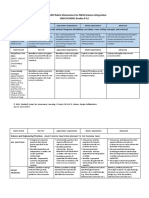
- Ngss Science Integration LDC 9-12 Rubric-3Dokumen6 halamanNgss Science Integration LDC 9-12 Rubric-3api-318937942Belum ada peringkat
- SAS - Session - 16.0 Research 2Dokumen3 halamanSAS - Session - 16.0 Research 2Angel Grace Palenso QuimzonBelum ada peringkat
- Approach Human: Ecosystem Health Glues Forget, Jean LebelDokumen40 halamanApproach Human: Ecosystem Health Glues Forget, Jean LebelBruno ImbroisiBelum ada peringkat
- Tylers Curriculum ModelDokumen15 halamanTylers Curriculum ModelchaBelum ada peringkat
- Measures of Central Tendency: Mean Median ModeDokumen20 halamanMeasures of Central Tendency: Mean Median ModeRia BarisoBelum ada peringkat
- HCLDokumen10 halamanHCLaakritiBelum ada peringkat
- Volcanoes - Abstract-Key WordsDokumen5 halamanVolcanoes - Abstract-Key WordsCarlos GuillenBelum ada peringkat
- Managerial EconomicsDokumen305 halamanManagerial EconomicsDeepu Deepak100% (5)
- Report On PureitDokumen21 halamanReport On Pureitsai govind kollethBelum ada peringkat
- PreviewpdfDokumen325 halamanPreviewpdfzerihun ayalewBelum ada peringkat
- MonographDokumen8 halamanMonographtaha shabanBelum ada peringkat
- Institutional Architecture Jan 2024Dokumen33 halamanInstitutional Architecture Jan 2024Rafael LeiteBelum ada peringkat
- Inquiries Investigations and Immersion LDokumen3 halamanInquiries Investigations and Immersion LJovel PaycanaBelum ada peringkat
- Measuring Dimensions and Density with CalipersDokumen3 halamanMeasuring Dimensions and Density with CalipersDorinneBarretto75% (4)
- Ule 2015Dokumen22 halamanUle 2015jhgfjgvjbhBelum ada peringkat
- Burnout in Organizational Life: Jonathon R.B. HalbeslebenDokumen21 halamanBurnout in Organizational Life: Jonathon R.B. HalbeslebenShaya RamrakhanBelum ada peringkat
- Teaching of SanskritDokumen2 halamanTeaching of SanskritBineet Kumar100% (2)
- Effects of Computer Among Children - Docx RealDokumen43 halamanEffects of Computer Among Children - Docx RealKiniBelum ada peringkat