Anda mungkin juga menyukai
- Classification Essay SampleDokumen3 halamanClassification Essay SampleAlvin Malquisto100% (2)
- NCLEX EndocrineDokumen21 halamanNCLEX EndocrineChristopher Harris100% (7)
- 07 MJN 24 (3) Nopphanath Et Al.Dokumen10 halaman07 MJN 24 (3) Nopphanath Et Al.Egy SunandaBelum ada peringkat
- Waist-to-Height Ratio Best Predicts DyslipidemiaDokumen6 halamanWaist-to-Height Ratio Best Predicts DyslipidemiaFitri annisaBelum ada peringkat
- Relationship of Body Mass Index With Lipid Profile Among Teaching Staff at The Higher Institute of Health Sciences, Sana'aDokumen6 halamanRelationship of Body Mass Index With Lipid Profile Among Teaching Staff at The Higher Institute of Health Sciences, Sana'aclaryntafreyaaBelum ada peringkat
- A Comparative Study of Association of Lipid Profile With Body Mass Index in General PopulationDokumen5 halamanA Comparative Study of Association of Lipid Profile With Body Mass Index in General PopulationIJAR JOURNALBelum ada peringkat
- CEREDA, 2013 - Anthropometric Indices of Fat Distribution and Cardiometabolic Risk in Parkinson's DiseaseDokumen8 halamanCEREDA, 2013 - Anthropometric Indices of Fat Distribution and Cardiometabolic Risk in Parkinson's DiseaseAndressa BurgosBelum ada peringkat
- Metabolic Syndrome in Adult Population of Rural Wardha, Central IndiaDokumen5 halamanMetabolic Syndrome in Adult Population of Rural Wardha, Central IndiaFebrian ParuraBelum ada peringkat
- 1 s2.0 S0378512223004516 MainDokumen9 halaman1 s2.0 S0378512223004516 MainTuyết mai ĐặngBelum ada peringkat
- Comparisons Between Anthropometric Indices For Predicting The Metabolic Syndrome in JapaneseDokumen6 halamanComparisons Between Anthropometric Indices For Predicting The Metabolic Syndrome in JapanesemkatoBelum ada peringkat
- Overwight Obesity PDFDokumen6 halamanOverwight Obesity PDFDebra1993Belum ada peringkat
- Body Mass Index Classification Misses Subjects With Increased Cardiometabolic Risk Factors Related To Elevated AdiposityDokumen9 halamanBody Mass Index Classification Misses Subjects With Increased Cardiometabolic Risk Factors Related To Elevated AdiposityHoài ThươngBelum ada peringkat
- CRP, Lipids, BMI Higher in Sudanese T2DM PatientsDokumen9 halamanCRP, Lipids, BMI Higher in Sudanese T2DM PatientsMotasem Sirag Mohmmed othmanBelum ada peringkat
- High Intensity Interval Training Is Not Superior To Contin - 2023 - Journal of EDokumen10 halamanHigh Intensity Interval Training Is Not Superior To Contin - 2023 - Journal of ESherriBelum ada peringkat
- 14 E10017 PDFDokumen4 halaman14 E10017 PDFNurul FajriBelum ada peringkat
- SCHWINGSHACKI2014Dokumen13 halamanSCHWINGSHACKI2014Saulo MartinsBelum ada peringkat
- 1 s2.0 S0954611113004137 MainDokumen7 halaman1 s2.0 S0954611113004137 MainPrama GitaBelum ada peringkat
- Diabetes - Saudi 3Dokumen7 halamanDiabetes - Saudi 3kalwusaidiBelum ada peringkat
- 268Dokumen6 halaman268ashwinbilagiBelum ada peringkat
- Relationship Between Obesity, Physical Activity, Sleeping Hours and Red Blood Cell Parameters in Adult Sudanese PopulationDokumen6 halamanRelationship Between Obesity, Physical Activity, Sleeping Hours and Red Blood Cell Parameters in Adult Sudanese Populationyuuki asunaBelum ada peringkat
- Art 6.vol 13 - 2 - 2013Dokumen6 halamanArt 6.vol 13 - 2 - 2013arc craftBelum ada peringkat
- Nutrients 12 01204Dokumen9 halamanNutrients 12 01204Ambusam SubramaniamBelum ada peringkat
- Correlation Between Waist and Mid-Thigh Circumference and Cardiovascular Fitness in Korean College Students: A Case StudyDokumen3 halamanCorrelation Between Waist and Mid-Thigh Circumference and Cardiovascular Fitness in Korean College Students: A Case StudyAndres CaceresBelum ada peringkat
- MTIwMTMxNDE PDFDokumen4 halamanMTIwMTMxNDE PDFMonica Herdiati Rukmana NaibahoBelum ada peringkat
- Roc en NutriciónDokumen15 halamanRoc en NutriciónTina MonroyBelum ada peringkat
- Anthropometric and Metabolic Indices in Assessment of Type and Severity of DyslipidemiaDokumen10 halamanAnthropometric and Metabolic Indices in Assessment of Type and Severity of DyslipidemiaferisiswonoBelum ada peringkat
- Effect of Aerobic Exercise On The Blood Lipid Profile in Young Adults PDFDokumen7 halamanEffect of Aerobic Exercise On The Blood Lipid Profile in Young Adults PDFCristian YanezBelum ada peringkat
- BackgroundDokumen16 halamanBackgroundDani KusumaBelum ada peringkat
- Significance of Skeletal Muscle Properties On Fitness, Long-Term Physical Training and Serum LipidsDokumen12 halamanSignificance of Skeletal Muscle Properties On Fitness, Long-Term Physical Training and Serum LipidsIrul AnwarBelum ada peringkat
- The Metabolic Syndrome: Comparison of Newly Proposed IDF, Modified ATP III and WHO Criteria and Their AgreementsDokumen6 halamanThe Metabolic Syndrome: Comparison of Newly Proposed IDF, Modified ATP III and WHO Criteria and Their AgreementsjoelBelum ada peringkat
- Correction Factors in METs ObeseDokumen5 halamanCorrection Factors in METs ObeseFranco Marin MUñozBelum ada peringkat
- Body Fat PercentageDokumen7 halamanBody Fat Percentagegurveer singhBelum ada peringkat
- Gater 2021Dokumen12 halamanGater 2021João Pedro PontesBelum ada peringkat
- Journal Article Cardiorespiratory FitnessDokumen19 halamanJournal Article Cardiorespiratory FitnessRekita DumpBelum ada peringkat
- Pancreatic Fat Deposition Is Increased and Related To Beta Cell Function in Women With Familial Partial LipodystrophyDokumen6 halamanPancreatic Fat Deposition Is Increased and Related To Beta Cell Function in Women With Familial Partial LipodystrophyThiago AlfradiqueBelum ada peringkat
- Artículo 5 - Sumatorio de Pliegues Subcutáneos Valores de Referencia para Atletas de ÉliteDokumen8 halamanArtículo 5 - Sumatorio de Pliegues Subcutáneos Valores de Referencia para Atletas de ÉliteEdward LozanoBelum ada peringkat
- Assessment of Body Composition and Serum Lipid Profile in School ChildrenDokumen6 halamanAssessment of Body Composition and Serum Lipid Profile in School Childrenproo213Belum ada peringkat
- Study of Lipid Profile in Shift WorkersDokumen6 halamanStudy of Lipid Profile in Shift WorkersDr Md Abedur Rahman100% (3)
- 2012 Obesity IndicesDokumen7 halaman2012 Obesity Indicesopolasek2Belum ada peringkat
- Correlation Entre Les Parametres Impedancemetriques Et Le Profil Lipidique Chez Des Patients Diabetiques de Type 2Dokumen9 halamanCorrelation Entre Les Parametres Impedancemetriques Et Le Profil Lipidique Chez Des Patients Diabetiques de Type 2IJAR JOURNALBelum ada peringkat
- Growth Status Among Females of Solan District of Himachal PradeshDokumen9 halamanGrowth Status Among Females of Solan District of Himachal PradeshDr. Krishna N. SharmaBelum ada peringkat
- Journal of Functional FoodsDokumen11 halamanJournal of Functional FoodsChintya JessicaBelum ada peringkat
- A Simple Cut Off For Waist To Height Ratio 05 Can Act As An Indicator For Cardiometabolic Risk Recent Data From Adults in The Health Survey For EnglandDokumen10 halamanA Simple Cut Off For Waist To Height Ratio 05 Can Act As An Indicator For Cardiometabolic Risk Recent Data From Adults in The Health Survey For Englandahmad aridoBelum ada peringkat
- Body Mass Index ObesityDokumen8 halamanBody Mass Index ObesityReyes Falcon D. ÁngelBelum ada peringkat
- TMP 37 D9Dokumen8 halamanTMP 37 D9FrontiersBelum ada peringkat
- Prema EtalDokumen6 halamanPrema EtaleditorijmrhsBelum ada peringkat
- Pone 0082853Dokumen10 halamanPone 0082853hyde93Belum ada peringkat
- Percent Body Fat Is A Better Predictor of Cardiovascular Risk Factors Than Body Mass IndexDokumen11 halamanPercent Body Fat Is A Better Predictor of Cardiovascular Risk Factors Than Body Mass IndexBrandon HeatBelum ada peringkat
- Pigłowska 2016Dokumen8 halamanPigłowska 2016Sam Steven Hernandez JañaBelum ada peringkat
- BMI Is Strongly Associated With Hypertension, and Waist Circumference in West ChinaDokumen7 halamanBMI Is Strongly Associated With Hypertension, and Waist Circumference in West ChinaAni RahmawatiBelum ada peringkat
- Role of Body Fat Loss in The Exercise-Induced Improvement of The Plasma Lipid Profile in Non-Insulin-Dependent Diabetes MellitusDokumen5 halamanRole of Body Fat Loss in The Exercise-Induced Improvement of The Plasma Lipid Profile in Non-Insulin-Dependent Diabetes MellitusSylvia ThohariBelum ada peringkat
- CARDIO METABOLIC RISK FACTORS AMONG POSTMENOPAUSAL SUDANESE WOMEN 17oct (1) Revision-TrackedDokumen28 halamanCARDIO METABOLIC RISK FACTORS AMONG POSTMENOPAUSAL SUDANESE WOMEN 17oct (1) Revision-Trackedhadiqa.iq95Belum ada peringkat
- Associations of BMI With All-Cause MortalityDokumen10 halamanAssociations of BMI With All-Cause MortalityainindyaBelum ada peringkat
- Correlation of CRP and Hypoalbuminemia With Morbid Obesity: Retrospective Study at KAUH, Jeddah, Saudi ArabiaDokumen9 halamanCorrelation of CRP and Hypoalbuminemia With Morbid Obesity: Retrospective Study at KAUH, Jeddah, Saudi ArabiaijasrjournalBelum ada peringkat
- JN7XX 17 PDFDokumen9 halamanJN7XX 17 PDFijasrjournalBelum ada peringkat
- Physiology & Behavior: SciencedirectDokumen8 halamanPhysiology & Behavior: SciencedirectScottBelum ada peringkat
- Exercise Intensity Prescription inDokumen8 halamanExercise Intensity Prescription inASHOK P KBelum ada peringkat
- Anthropometric Correlates of Blood Pressure in Normotensive Pakistani SubjectsDokumen4 halamanAnthropometric Correlates of Blood Pressure in Normotensive Pakistani SubjectsMohamed MansourBelum ada peringkat
- 2017 Article 2868Dokumen9 halaman2017 Article 2868Yigit İskurtBelum ada peringkat
- Vit D, Metabolic Syndrome Study in KoreaDokumen8 halamanVit D, Metabolic Syndrome Study in Koreatrisna amijayaBelum ada peringkat
- Ba LacedDokumen4 halamanBa LacedRubini Devi MutthusamyBelum ada peringkat
- Exercise Physiology for the Pediatric and Congenital CardiologistDari EverandExercise Physiology for the Pediatric and Congenital CardiologistBelum ada peringkat
- 587f12ab80e85 PDFDokumen125 halaman587f12ab80e85 PDFamira catriBelum ada peringkat
- 1804200832_2017_Nommensen Journal of Medicine Vol 3 No 1 Juli 2017_6. Hubungan Indeks Massa Tubuh Dengan Profil Lipid Serum Sebagai Faktor Risiko Penyakit Kardiovaskuler Pada Mahasiswa Universitas HKBP Nommensen(1)Dokumen7 halaman1804200832_2017_Nommensen Journal of Medicine Vol 3 No 1 Juli 2017_6. Hubungan Indeks Massa Tubuh Dengan Profil Lipid Serum Sebagai Faktor Risiko Penyakit Kardiovaskuler Pada Mahasiswa Universitas HKBP Nommensen(1)amira catriBelum ada peringkat
- Digital 124623 S09052fk Prevalens Obesitas BibliografiDokumen3 halamanDigital 124623 S09052fk Prevalens Obesitas Bibliografiamira catriBelum ada peringkat
- Perbedaan Profil Lipid Pada Remaja Obes Dan Tidak Obes Di Kecamatan Bolangitang BaratDokumen8 halamanPerbedaan Profil Lipid Pada Remaja Obes Dan Tidak Obes Di Kecamatan Bolangitang Baratamira catriBelum ada peringkat
- Digital 122846 S09039fk Prevalens Obesitas BibliografiDokumen2 halamanDigital 122846 S09039fk Prevalens Obesitas Bibliografiamira catriBelum ada peringkat
- Faktor Risiko Kegemukan Pada Wanita Dewasa Indonesia: ISSN 1978 - 1059 Jurnal Gizi Dan Pangan, Maret 2013, 8 (1) : 1-8Dokumen8 halamanFaktor Risiko Kegemukan Pada Wanita Dewasa Indonesia: ISSN 1978 - 1059 Jurnal Gizi Dan Pangan, Maret 2013, 8 (1) : 1-8IrmadaniBelum ada peringkat
- 279 627 1 PBDokumen10 halaman279 627 1 PBWalter WattsBelum ada peringkat
- Factors Associated with Obesity in Police Officers in Pontianak CityDokumen14 halamanFactors Associated with Obesity in Police Officers in Pontianak Cityamira catriBelum ada peringkat
- Guia Practica Fa 2016Dokumen90 halamanGuia Practica Fa 2016Juan Carlos SuarezBelum ada peringkat
- The Asia Pacific Heart Rhythm Society Guidelines: Venice Arrhythmias 2015Dokumen39 halamanThe Asia Pacific Heart Rhythm Society Guidelines: Venice Arrhythmias 2015amira catriBelum ada peringkat
- 62 129 1 SM PDFDokumen4 halaman62 129 1 SM PDFDesinta Mitha SariBelum ada peringkat
- Hepatitis A Virus Infection and Hepatitis A Vaccination in Human Immunodeficiency Virus-Positive Patients: A ReviewDokumen19 halamanHepatitis A Virus Infection and Hepatitis A Vaccination in Human Immunodeficiency Virus-Positive Patients: A Reviewamira catriBelum ada peringkat
- Optimisme Kesembuhan Pada Penderita Mioma UteriDokumen13 halamanOptimisme Kesembuhan Pada Penderita Mioma UteriSyah DiyahBelum ada peringkat
- Respiratory Quotient: Method of Determination: USING RESPIROMETERDokumen4 halamanRespiratory Quotient: Method of Determination: USING RESPIROMETERNeethi KrishnanBelum ada peringkat
- Katalyst Fitness Opens Third Studio: The World's Most Efficient Workout Is Now Available in The United StatesDokumen2 halamanKatalyst Fitness Opens Third Studio: The World's Most Efficient Workout Is Now Available in The United StatesPR.comBelum ada peringkat
- Risk Factors: What Are The Risk Factors For Colorectal Cancer?Dokumen2 halamanRisk Factors: What Are The Risk Factors For Colorectal Cancer?Dinda AriestaBelum ada peringkat
- What Is NutrigenomicsDokumen6 halamanWhat Is NutrigenomicsRitu AilaniBelum ada peringkat
- Cancer Genetics Signature Assignment Part 1 Article No. 1: TV Raises Blood Pressure in Obese Kids: StudyDokumen3 halamanCancer Genetics Signature Assignment Part 1 Article No. 1: TV Raises Blood Pressure in Obese Kids: StudyLancer HopBelum ada peringkat
- Inles 4Dokumen2 halamanInles 4Astrid CruzBelum ada peringkat
- Calculate Total Energy and Nutrient DistributionDokumen11 halamanCalculate Total Energy and Nutrient Distributiondorothy0% (1)
- Once Again A Vegan Centenarian Is The Nation's Oldest Man! - 112 Year Old Pandit Sudhakar Chaturvedi - Not Paleo, Low Carb, Wheat Belly, Atkins, But VegetarianDokumen3 halamanOnce Again A Vegan Centenarian Is The Nation's Oldest Man! - 112 Year Old Pandit Sudhakar Chaturvedi - Not Paleo, Low Carb, Wheat Belly, Atkins, But VegetarianPaleoCentenarianDiet33% (3)
- The artery most likely to be eroded in perforation of the posterior wall of the first part of the duodenum is the superior pancreaticoduodenal artery. It is a branch of the gastroduodenal arteryDokumen33 halamanThe artery most likely to be eroded in perforation of the posterior wall of the first part of the duodenum is the superior pancreaticoduodenal artery. It is a branch of the gastroduodenal arteryWahida Amalin Ab RazakBelum ada peringkat
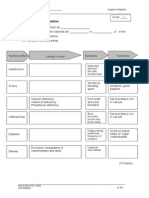
- WORKSHEET 6.3 MalnutritionDokumen4 halamanWORKSHEET 6.3 MalnutritionLim Wai Wai SmktpBelum ada peringkat
- Entrenamiento IsoinercialDokumen9 halamanEntrenamiento IsoinercialVictor Andrés Olivares IbarraBelum ada peringkat
- SpecForce Alpha Program Turns You Into an Elite OperatorDokumen52 halamanSpecForce Alpha Program Turns You Into an Elite OperatorIanBelum ada peringkat
- Lab Assignment: Community Nutrition BS-III (6 Semester)Dokumen23 halamanLab Assignment: Community Nutrition BS-III (6 Semester)huzairaBelum ada peringkat
- 10 Tips for Starting Your Wellness Journey TodayDokumen7 halaman10 Tips for Starting Your Wellness Journey TodayEzzah SobliBelum ada peringkat
- Organic Food No More Nutritious: 1. GAP FILL: Put The Words Into The Gaps in The TextDokumen3 halamanOrganic Food No More Nutritious: 1. GAP FILL: Put The Words Into The Gaps in The TextCompañia de Maria -antiguas alumnas-100% (1)
- Gabriel Gonzaga's Mother's Life Expectancy: 82 Years According to SurveyDokumen2 halamanGabriel Gonzaga's Mother's Life Expectancy: 82 Years According to SurveyRizza Gonzaga100% (2)
- Kurva Z Score WhoDokumen21 halamanKurva Z Score WhoFenty IswarBelum ada peringkat
- Graphing ActivitiesDokumen12 halamanGraphing Activitiesapi-292104717Belum ada peringkat
- Vazhakoombu: Kerala's famous banana variety has intrinsic health benefitsDokumen2 halamanVazhakoombu: Kerala's famous banana variety has intrinsic health benefitsKanishk KatareBelum ada peringkat
- Hibah FK UGM - Hongkong Publication Blood Lead Level - Sudargo, Ma'Rifah, Zakia, Sari, Hariawan, PramasthiDokumen6 halamanHibah FK UGM - Hongkong Publication Blood Lead Level - Sudargo, Ma'Rifah, Zakia, Sari, Hariawan, PramasthiDea Farah ZakiaBelum ada peringkat
- Mechanisms Behind Blood Flow Restricted Training and Its Effect Towards Muscle GrowthDokumen40 halamanMechanisms Behind Blood Flow Restricted Training and Its Effect Towards Muscle GrowthFranciscoJavierRoblesBelum ada peringkat
- Carbohydrates, Sugars, Starches and Fiber: © 2010 Pearson Education, IncDokumen67 halamanCarbohydrates, Sugars, Starches and Fiber: © 2010 Pearson Education, IncCharlette E. NavarrosaBelum ada peringkat
- Vomiting in ChildrenDokumen41 halamanVomiting in ChildrenWiresa RenaltaBelum ada peringkat
- LAMIGAS - BSN2H-Laboratory No. 2Dokumen3 halamanLAMIGAS - BSN2H-Laboratory No. 2Juliemae LamigasBelum ada peringkat
- Pe and HealthDokumen29 halamanPe and Healthvan dulayBelum ada peringkat
- 1st Adime - HWDokumen3 halaman1st Adime - HWapi-243208495Belum ada peringkat
- Effect of BMI on complications in thoracic surgeryDokumen9 halamanEffect of BMI on complications in thoracic surgeryNoviBelum ada peringkat
- Benefits and Risks of The Keto DietDokumen3 halamanBenefits and Risks of The Keto DietSaurabh PandeyBelum ada peringkat