Anda mungkin juga menyukai
- Opioid Use Disorders:: Therapeutic Manuals for Healing and RecuperationDari EverandOpioid Use Disorders:: Therapeutic Manuals for Healing and RecuperationBelum ada peringkat
- Warfarin, Insulin and Digoxin Are The Most Dangerous Drugs in The Elderly. Do We Believe That?Dokumen32 halamanWarfarin, Insulin and Digoxin Are The Most Dangerous Drugs in The Elderly. Do We Believe That?pinkbutterBelum ada peringkat
- Adverse Drug ReactionDokumen24 halamanAdverse Drug ReactionGopal pokhrelBelum ada peringkat
- BY: Antira Anisahati, S.Farm., AptDokumen18 halamanBY: Antira Anisahati, S.Farm., AptRetno puspitariniBelum ada peringkat
- Risk Factors For Cutaneous Adverse Drug ReactionsDokumen26 halamanRisk Factors For Cutaneous Adverse Drug ReactionsMukesh Kumar SharmaBelum ada peringkat
- Warfarin, Insulin and Digoxin Are The Most Dangerous Drugs in The Elderly. Do We Believe That?Dokumen32 halamanWarfarin, Insulin and Digoxin Are The Most Dangerous Drugs in The Elderly. Do We Believe That?kirana_patrolinaBelum ada peringkat
- ADR, Monitoring& ReportingDokumen24 halamanADR, Monitoring& ReportingMerlin DineshBelum ada peringkat
- Review On Adverse Drug Reactions 2167 1052.1000005 RDokumen2 halamanReview On Adverse Drug Reactions 2167 1052.1000005 RSourabh kundaraBelum ada peringkat
- Adverse Drug ReactionsDokumen32 halamanAdverse Drug ReactionsIrum ChohanBelum ada peringkat
- Warfarin, Insulin and Digoxin Are The Most Dangerous Drugs in The Elderly. Do We Believe That?Dokumen32 halamanWarfarin, Insulin and Digoxin Are The Most Dangerous Drugs in The Elderly. Do We Believe That?Zarish IftikharBelum ada peringkat
- Lecture 5 PharmacovigilanceDokumen32 halamanLecture 5 Pharmacovigilancephoto copyhemnBelum ada peringkat
- Pharmacovigilance V01Dokumen33 halamanPharmacovigilance V01Karveer AghadeBelum ada peringkat
- Adverse Drug Reactions: Key PointsDokumen6 halamanAdverse Drug Reactions: Key PointsOvi RifaniBelum ada peringkat
- Adverse Drug Reactions 23 24 1Dokumen37 halamanAdverse Drug Reactions 23 24 1Hasan kahhalehBelum ada peringkat
- Adverse Drug Events, Reactions and Errors FAQsDokumen1 halamanAdverse Drug Events, Reactions and Errors FAQsNavodit ThakralBelum ada peringkat
- 1.adverse Drug ReactionDokumen42 halaman1.adverse Drug ReactionSV. Trần Hữu ThắngBelum ada peringkat
- Adr PDFDokumen9 halamanAdr PDFdewi atmajaBelum ada peringkat
- Adverse Eeffects of Drugs and Their Management in PaediatricsDokumen6 halamanAdverse Eeffects of Drugs and Their Management in PaediatricsRinchin ChhotenBelum ada peringkat
- The Principles of Drugs Prescribing & Drug InteractionDokumen87 halamanThe Principles of Drugs Prescribing & Drug InteractionRastia AlimmattabrinaBelum ada peringkat
- A Presentation On Adr Due To AntibioitcsDokumen18 halamanA Presentation On Adr Due To AntibioitcsAnta SharmaBelum ada peringkat
- Adverse Eeffects of Drugs and Their Management in PaediatricsDokumen6 halamanAdverse Eeffects of Drugs and Their Management in PaediatricsRinchin ChhotenBelum ada peringkat
- 71128lecture 4Dokumen25 halaman71128lecture 4azizBelum ada peringkat
- Ksmu Department of Clinical PharmacologyDokumen15 halamanKsmu Department of Clinical PharmacologyLucas Victor AlmeidaBelum ada peringkat
- Tinjauan Pustaka: Adverse Drug ReactionDokumen9 halamanTinjauan Pustaka: Adverse Drug Reactionzulfaningsih HSBelum ada peringkat
- Adverse Drug ReactionDokumen30 halamanAdverse Drug ReactionSophia AndresBelum ada peringkat
- Clinical Pharmacy: By: Narendar KumarDokumen14 halamanClinical Pharmacy: By: Narendar KumarAlee Iz HarBelum ada peringkat
- 6 ABC of Drug-Related Problems PDFDokumen9 halaman6 ABC of Drug-Related Problems PDFMadalinaMadaBelum ada peringkat
- ADRs, Reporting and Causality AssessmentDokumen37 halamanADRs, Reporting and Causality AssessmentRaymond ManjengwaBelum ada peringkat
- Understanding Medicine Side Effects and DangersDokumen12 halamanUnderstanding Medicine Side Effects and DangersmutiaraBelum ada peringkat
- General - Principle - of - Pharmacology 3Dokumen7 halamanGeneral - Principle - of - Pharmacology 3Ntando MdhluliBelum ada peringkat
- CR 1.pdfDokumen22 halamanCR 1.pdftyleree3Belum ada peringkat
- Phar 5 6-7Dokumen4 halamanPhar 5 6-7Clay BakerBelum ada peringkat
- Adverse Drug ReactionsDokumen5 halamanAdverse Drug Reactionswjraffle2Belum ada peringkat
- Adrs 150226194556 Conversion Gate02Dokumen56 halamanAdrs 150226194556 Conversion Gate02Ayu WijiBelum ada peringkat
- Adverse Drug Reactions ADR Classes ADR Reporting ADRDokumen37 halamanAdverse Drug Reactions ADR Classes ADR Reporting ADRMahum SohailBelum ada peringkat
- Chapter 4: Implementing The Pharmacists' Patient Care ProcessDokumen15 halamanChapter 4: Implementing The Pharmacists' Patient Care ProcessLouise TheunisBelum ada peringkat
- Adverse Drug ReactionsDokumen14 halamanAdverse Drug Reactionsgaikwaduv98Belum ada peringkat
- Lecture (6) - ADRs MonitoringDokumen38 halamanLecture (6) - ADRs MonitoringRaju NiraulaBelum ada peringkat
- Brief Notes On PharmacovigilanceDokumen78 halamanBrief Notes On Pharmacovigilancejay100% (1)
- Pharmacokinetic and pharmacodynamic drug interactionsDokumen55 halamanPharmacokinetic and pharmacodynamic drug interactionsElinor QuintoBelum ada peringkat
- Guidance On Adverse Drug ReactionsDokumen5 halamanGuidance On Adverse Drug Reactionssoraoto arashinaBelum ada peringkat
- ADR Monitoring and ReportingDokumen13 halamanADR Monitoring and ReportingKinjal GamitBelum ada peringkat
- PharmacologyDokumen5 halamanPharmacologySaqline MondalBelum ada peringkat
- Medication Error 2017Dokumen51 halamanMedication Error 2017Christina100% (1)
- ADR Final1Dokumen10 halamanADR Final1Rubina BisankheBelum ada peringkat
- 68w Chapter 3 - RevDokumen8 halaman68w Chapter 3 - Revsmith.kevin1420344Belum ada peringkat
- PHARMACOVIGILANCEDokumen15 halamanPHARMACOVIGILANCEmanveer84100% (3)
- Medication SafetyDokumen54 halamanMedication SafetyJuwitaASih100% (2)
- Presentasi PC To Prevent MEDokumen39 halamanPresentasi PC To Prevent MEAkhmad Rafi'iBelum ada peringkat
- Adr NewDokumen43 halamanAdr Newshyamsundermaurya987Belum ada peringkat
- Medication Safety TerminologyDokumen25 halamanMedication Safety TerminologyAnwar SallehBelum ada peringkat
- Medication and transfusion errors indicatorsDokumen11 halamanMedication and transfusion errors indicatorsYogesh ChandraBelum ada peringkat
- Adverse Drug Reactions ExplainedDokumen108 halamanAdverse Drug Reactions ExplainedBinod Sah100% (2)
- Pharmacists in Patient CareDokumen47 halamanPharmacists in Patient CaremekuriawBelum ada peringkat
- Clinical Pharmacy Complete Notes-CompressedDokumen355 halamanClinical Pharmacy Complete Notes-CompressedM. Huzaifa Nasir100% (1)
- Side Effects of drugs, ABCDE ClassificationDokumen33 halamanSide Effects of drugs, ABCDE ClassificationonyekaBelum ada peringkat
- Adr & Di PDFDokumen30 halamanAdr & Di PDFSri SriBelum ada peringkat
- Irfan Ahmad Khan Assistant Professor Dept of PharmacDokumen34 halamanIrfan Ahmad Khan Assistant Professor Dept of PharmacShubhamBelum ada peringkat
- Pharmacology Group 3Dokumen9 halamanPharmacology Group 3wiyadiBelum ada peringkat
- Chapter 7 CapsulesDokumen87 halamanChapter 7 CapsulesTeresa Saylo92% (26)
- Pharmaceutical Merits&Demerits of EmulsionDokumen6 halamanPharmaceutical Merits&Demerits of EmulsionShemaj GurchumaBelum ada peringkat
- File 1Dokumen5 halamanFile 1Sk AslamBelum ada peringkat
- Quality Tests for Oral Drug ProductsDokumen8 halamanQuality Tests for Oral Drug ProductssfgvsdfrbhBelum ada peringkat
- Para Modificar AgentspyDokumen5 halamanPara Modificar AgentspyIvanBelum ada peringkat
- PPhA 2016 CPD Seminar ScheduleDokumen1 halamanPPhA 2016 CPD Seminar ScheduleAre Pee EtcBelum ada peringkat
- Activities For Community PharmacyDokumen12 halamanActivities For Community Pharmacycjh1015960% (1)
- ICH Q12 Guideline on Pharmaceutical Product Lifecycle ManagementDokumen23 halamanICH Q12 Guideline on Pharmaceutical Product Lifecycle ManagementrezaBelum ada peringkat
- Age Appropriate Dosage For ChildrenDokumen22 halamanAge Appropriate Dosage For Childrenmukesh choudharyBelum ada peringkat
- Introduction To Pharma LecDokumen22 halamanIntroduction To Pharma LecFrancis Polycarp DiazBelum ada peringkat
- Drug Development Process - Part 4 PDFDokumen5 halamanDrug Development Process - Part 4 PDFNguyễn Thế ThaoBelum ada peringkat
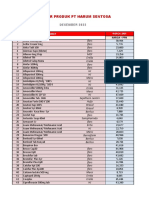
- Daftar Produk PT Harum Sentosa: NO Nama ObatDokumen10 halamanDaftar Produk PT Harum Sentosa: NO Nama ObatLutfia LatifahBelum ada peringkat
- Obat2 PentingDokumen1 halamanObat2 PentingMuhammad Satya EnzoBelum ada peringkat
- House Democrats Request Information From FDA On Aduhelm ApprovalDokumen13 halamanHouse Democrats Request Information From FDA On Aduhelm ApprovalRachel CohrsBelum ada peringkat
- Dispensing Fee Report All Provinces Except OnDokumen66 halamanDispensing Fee Report All Provinces Except OnVladislav KrasovskyBelum ada peringkat
- PHRM 246: MR Thabiso Tlaila Department of Pharmacology Discipline of Pharmaceutical Sciences University of Kwazulu-NatalDokumen38 halamanPHRM 246: MR Thabiso Tlaila Department of Pharmacology Discipline of Pharmaceutical Sciences University of Kwazulu-NatalSindile MchunuBelum ada peringkat
- Apotek Saufifi ListDokumen28 halamanApotek Saufifi ListFikriYTBelum ada peringkat
- DissolutionDokumen29 halamanDissolutionLama QaimariBelum ada peringkat
- Dias2009 Article PantoprazoleDokumen10 halamanDias2009 Article PantoprazoleTan JayBelum ada peringkat
- Registered Pharmacist Self DeclarationDokumen1 halamanRegistered Pharmacist Self DeclarationShraddha Piyush Agrawal100% (2)
- Thyme Increase The Levothyroxine Dose by 30-50%: This Is For Mild To Moderate But For Severe We Will Give Him TriptansDokumen66 halamanThyme Increase The Levothyroxine Dose by 30-50%: This Is For Mild To Moderate But For Severe We Will Give Him TriptansOuf'ra AbdulmajidBelum ada peringkat
- CiteLtr - Smetana, James W., R.PHDokumen3 halamanCiteLtr - Smetana, James W., R.PHJames LindonBelum ada peringkat
- Pharmacology (DNPC 4122) Topic: Type of Medication Route: Presented byDokumen22 halamanPharmacology (DNPC 4122) Topic: Type of Medication Route: Presented bySuhaimi ShafieBelum ada peringkat
- Pengantar Ilmu FarmasiDokumen13 halamanPengantar Ilmu FarmasinabilaBelum ada peringkat
- Ahfs 2011 Hidroksizine HidrokloridaDokumen5 halamanAhfs 2011 Hidroksizine HidrokloridaDiny AnisaBelum ada peringkat
- Adverse EffectsDokumen27 halamanAdverse EffectsNoha AzzamBelum ada peringkat
- Mariano Que's Rags-to-Riches StoryDokumen8 halamanMariano Que's Rags-to-Riches StoryEunise Punzalan OprinBelum ada peringkat
- Exercise 6.pdf 94259Dokumen4 halamanExercise 6.pdf 94259Loli HunterBelum ada peringkat
- Format RKO Dan RKBMHP 2024.xlsx KEMUSUDokumen40 halamanFormat RKO Dan RKBMHP 2024.xlsx KEMUSUWatik Nurul FaizahBelum ada peringkat
- PharmacyDokumen13 halamanPharmacykaveesh_93Belum ada peringkat