Anda mungkin juga menyukai
- 1 s2.0 S106474062100078XDokumen8 halaman1 s2.0 S106474062100078XTrnrFdy ViveroBelum ada peringkat
- BSRD Tooth Wear BookletDokumen28 halamanBSRD Tooth Wear BookletSalma RafiqBelum ada peringkat
- TALLER 4selwitz2007Dokumen9 halamanTALLER 4selwitz2007Natalia SplashBelum ada peringkat
- Periodontal EmergenciesDokumen7 halamanPeriodontal Emergenciesnandi prasetyaBelum ada peringkat
- Periodontal Emergencies in General Practice: Primary Dental Journal June 2017Dokumen7 halamanPeriodontal Emergencies in General Practice: Primary Dental Journal June 2017AmadeaBelum ada peringkat
- Pedodontic Lect 17Dokumen10 halamanPedodontic Lect 17Mustafa AmmarBelum ada peringkat
- Predictable Management of Cracked Teeth With Reversible PulpitisDokumen10 halamanPredictable Management of Cracked Teeth With Reversible PulpitisNaji Z. ArandiBelum ada peringkat
- CYSTSDokumen12 halamanCYSTSGowriBelum ada peringkat
- Eruptive Disorders of Permanent TeethDokumen6 halamanEruptive Disorders of Permanent Teethtaliya. shvetzBelum ada peringkat
- Endo-Perio Continuum A Review From Cause To CureDokumen4 halamanEndo-Perio Continuum A Review From Cause To CureRiezaBelum ada peringkat
- Aggressive Periodontitis: Case Definition and Diagnostic CriteriaDokumen15 halamanAggressive Periodontitis: Case Definition and Diagnostic Criteriadileep9002392Belum ada peringkat
- Denture Stomatitis: Causes, Cures and PreventionDokumen6 halamanDenture Stomatitis: Causes, Cures and PreventionUlip KusumaBelum ada peringkat
- Presentation2 Impaction (Online)Dokumen91 halamanPresentation2 Impaction (Online)lola abualillBelum ada peringkat
- Ajohas 3 5 2Dokumen7 halamanAjohas 3 5 2Ega Id'ham pramudyaBelum ada peringkat
- Dental Cariesthe LancetDokumen10 halamanDental Cariesthe LancetManari CatalinaBelum ada peringkat
- DentalCariestheLancet PDFDokumen10 halamanDentalCariestheLancet PDFManari CatalinaBelum ada peringkat
- Benign and MalignantDokumen16 halamanBenign and MalignantRSU DUTA MULYABelum ada peringkat
- Vertical Root Fracture !Dokumen42 halamanVertical Root Fracture !Dr Dithy kkBelum ada peringkat
- Jper 17-0733Dokumen12 halamanJper 17-0733Jonathan Meza MauricioBelum ada peringkat
- 8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethDokumen8 halaman8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethAhmed AbdBelum ada peringkat
- Chronic Suppurative Osteomyelitis of The Mandible CaseDokumen4 halamanChronic Suppurative Osteomyelitis of The Mandible Caseporsche_cruiseBelum ada peringkat
- SJ BDJ 2013 1192Dokumen6 halamanSJ BDJ 2013 1192Fadhil MiftahulBelum ada peringkat
- Sidang Tesis TGL 30 Oktober 2014 Final FixedDokumen11 halamanSidang Tesis TGL 30 Oktober 2014 Final Fixedfaizal prabowo KalimanBelum ada peringkat
- Periodontics PDFDokumen195 halamanPeriodontics PDFدينا حسن نعمة100% (1)
- Jurnal PedoDokumen4 halamanJurnal PedoMantika AtiqahBelum ada peringkat
- Lec 1 Diagnosis and Mouth PreparationDokumen10 halamanLec 1 Diagnosis and Mouth PreparationAhmad MesaedBelum ada peringkat
- Covid-19 Impact An Oral Health With A Focus On Temporomandibular Joint DisordersDokumen5 halamanCovid-19 Impact An Oral Health With A Focus On Temporomandibular Joint Disordersbotak berjamaahBelum ada peringkat
- Mucogingival Conditions in The Natural DentitionDokumen9 halamanMucogingival Conditions in The Natural Dentitionclaudyedith197527Belum ada peringkat
- JInterdiscipDentistry12119-4138785 112947 PDFDokumen6 halamanJInterdiscipDentistry12119-4138785 112947 PDFAndamiaBelum ada peringkat
- Pratica 2Dokumen5 halamanPratica 2Emiliano ArrietaBelum ada peringkat
- Periodontal Emergencies Article 2017Dokumen6 halamanPeriodontal Emergencies Article 2017abdslam leilaBelum ada peringkat
- 5 Management of Internal RootDokumen5 halaman5 Management of Internal RootDana StanciuBelum ada peringkat
- Eb 79Dokumen5 halamanEb 79mohammad naufalBelum ada peringkat
- Jurnal Resesi 6Dokumen4 halamanJurnal Resesi 6viena mutmainnahBelum ada peringkat
- Internal ResorptionDokumen4 halamanInternal ResorptionmaharaniBelum ada peringkat
- Time To Shift - From Scaling and Root Planing To Root Surface DebridementDokumen5 halamanTime To Shift - From Scaling and Root Planing To Root Surface DebridementYing Yi TeoBelum ada peringkat
- Extreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical ManagementDokumen8 halamanExtreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical Managementcarmen espinozaBelum ada peringkat
- Acute Periodontal LesionsDokumen30 halamanAcute Periodontal LesionsIbán CruzBelum ada peringkat
- Oral Ulceration: GP Guide To Diagnosis and Treatment: Stephen Flint Ma, PHD, MB BS, BDS, FDSRCS, Ffdrcsi, FicdDokumen9 halamanOral Ulceration: GP Guide To Diagnosis and Treatment: Stephen Flint Ma, PHD, MB BS, BDS, FDSRCS, Ffdrcsi, FicdEstuBelum ada peringkat
- The Periodontal Abscess: A ReviewDokumen10 halamanThe Periodontal Abscess: A ReviewRENATO SUDATIBelum ada peringkat
- Pulp Therapy For Primary Molars-UK GuidelinesDokumen9 halamanPulp Therapy For Primary Molars-UK GuidelinesRania AghaBelum ada peringkat
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDokumen6 halamanEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargBelum ada peringkat
- Complex Crown Fracture Presenting 5 Hours Post Trauma in A General Dental PracticeDokumen8 halamanComplex Crown Fracture Presenting 5 Hours Post Trauma in A General Dental PracticeKamel ArgoubiBelum ada peringkat
- Mucogingival Conditions in The Natural DentitionDokumen10 halamanMucogingival Conditions in The Natural DentitionMartty BaBelum ada peringkat
- Niemiec 2009Dokumen16 halamanNiemiec 2009Bryan Sebastian Valdez MorejónBelum ada peringkat
- Dafpus 1Dokumen8 halamanDafpus 1Winda WidhyastutiBelum ada peringkat
- Ndodontic Iagnosis: by Clifford J. Ruddle, D.D.SDokumen10 halamanNdodontic Iagnosis: by Clifford J. Ruddle, D.D.Srojek63Belum ada peringkat
- An Alternative Method For Splinting of PDFDokumen5 halamanAn Alternative Method For Splinting of PDFRamona MateiBelum ada peringkat
- Int Endodontic J - 2022 - Abbott - Present Status and Future Directions Managing Endodontic EmergenciesDokumen26 halamanInt Endodontic J - 2022 - Abbott - Present Status and Future Directions Managing Endodontic EmergenciesRazvan UngureanuBelum ada peringkat
- The Risk of Healing Complications in Primary Teeth With Root FracturesDokumen7 halamanThe Risk of Healing Complications in Primary Teeth With Root FracturesRazvan UngureanuBelum ada peringkat
- Jurnal 2 Scalloped TongueDokumen3 halamanJurnal 2 Scalloped TonguestephanieBelum ada peringkat
- Endo-Perio Lesions Diagnosis and Clinical ConsiderationsDokumen8 halamanEndo-Perio Lesions Diagnosis and Clinical ConsiderationsBejan OvidiuBelum ada peringkat
- Content ServerDokumen7 halamanContent ServerJUAN DIEGO DUARTE VILLARREALBelum ada peringkat
- Perio PBLKasvuGingivalOvergrowthDokumen32 halamanPerio PBLKasvuGingivalOvergrowthDraspiBelum ada peringkat
- Dental Radiology LectureDokumen40 halamanDental Radiology LectureAbdullahayad farouqBelum ada peringkat
- Jurnal CRSS Prothesa 4 (Sixna Agitha Claresta 20204020100)Dokumen7 halamanJurnal CRSS Prothesa 4 (Sixna Agitha Claresta 20204020100)sixnaagithaBelum ada peringkat
- NakamuraDokumen11 halamanNakamuraMairaMaraviChavezBelum ada peringkat
- Gujral FCMDokumen102 halamanGujral FCMcandiddreamsBelum ada peringkat
- Clinical Biomechanics: Leigh W. Marshall, Stuart M. McgillDokumen4 halamanClinical Biomechanics: Leigh W. Marshall, Stuart M. McgillMichael JunBelum ada peringkat
- Warehouse Management Solution SheetDokumen2 halamanWarehouse Management Solution Sheetpatelnandini109Belum ada peringkat
- DJI F450 Construction Guide WebDokumen21 halamanDJI F450 Construction Guide WebPutu IndrayanaBelum ada peringkat
- Arts Class: Lesson 01Dokumen24 halamanArts Class: Lesson 01Lianne BryBelum ada peringkat
- Aquaculture Scoop May IssueDokumen20 halamanAquaculture Scoop May IssueAquaculture ScoopBelum ada peringkat
- B737-3 ATA 23 CommunicationsDokumen112 halamanB737-3 ATA 23 CommunicationsPaul RizlBelum ada peringkat
- CCNA Training New CCNA - RSTPDokumen7 halamanCCNA Training New CCNA - RSTPokotete evidenceBelum ada peringkat
- Anderson, Poul - Flandry 02 - A Circus of HellsDokumen110 halamanAnderson, Poul - Flandry 02 - A Circus of Hellsgosai83Belum ada peringkat
- ACR39U-U1: (USB Type A) Smart Card ReaderDokumen8 halamanACR39U-U1: (USB Type A) Smart Card Readersuraj18in4uBelum ada peringkat
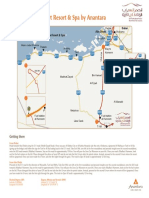
- Qasr Al Sarab Desert Resort Location Map June2012Dokumen1 halamanQasr Al Sarab Desert Resort Location Map June2012Anant GârgBelum ada peringkat
- Case 445Dokumen4 halamanCase 445ForomaquinasBelum ada peringkat
- Kinder DLL Week 8Dokumen15 halamanKinder DLL Week 8Jainab Pula SaiyadiBelum ada peringkat
- Discrete Wavelet TransformDokumen10 halamanDiscrete Wavelet TransformVigneshInfotechBelum ada peringkat
- Keyword 4: Keyword: Strength of The Mixture of AsphaltDokumen2 halamanKeyword 4: Keyword: Strength of The Mixture of AsphaltJohn Michael GeneralBelum ada peringkat
- The Indian & The SnakeDokumen3 halamanThe Indian & The SnakeashvinBelum ada peringkat
- FactSet London OfficeDokumen1 halamanFactSet London OfficeDaniyar KaliyevBelum ada peringkat
- Ict 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Dokumen14 halamanIct 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Chiropractic Marketing NowBelum ada peringkat
- Pharmalytica Exhibitor List 2023Dokumen3 halamanPharmalytica Exhibitor List 2023Suchita PoojaryBelum ada peringkat
- Principles Involved in Baking 1Dokumen97 halamanPrinciples Involved in Baking 1Milky BoyBelum ada peringkat
- Danika Cristoal 18aDokumen4 halamanDanika Cristoal 18aapi-462148990Belum ada peringkat
- AppearancesDokumen4 halamanAppearancesReme TrujilloBelum ada peringkat
- Quartile1 PDFDokumen2 halamanQuartile1 PDFHanifah Edres DalumaBelum ada peringkat
- 1 s2.0 S1110016815000563 Main PDFDokumen13 halaman1 s2.0 S1110016815000563 Main PDFvale1299Belum ada peringkat
- Conceptual Artist in Nigeria UNILAGDokumen13 halamanConceptual Artist in Nigeria UNILAGAdelekan FortuneBelum ada peringkat
- Cold Regions Science and TechnologyDokumen8 halamanCold Regions Science and TechnologyAbraham SilesBelum ada peringkat
- English2 Q2 Summative Assessment 4 2Dokumen4 halamanEnglish2 Q2 Summative Assessment 4 2ALNIE PANGANIBANBelum ada peringkat
- W0L0XCF0866101640 (2006 Opel Corsa) PDFDokumen7 halamanW0L0XCF0866101640 (2006 Opel Corsa) PDFgianyBelum ada peringkat
- The Manufacture and Uses of Expanded Clay Aggregate: Thursday 15 November 2012 SCI HQ, LondonDokumen36 halamanThe Manufacture and Uses of Expanded Clay Aggregate: Thursday 15 November 2012 SCI HQ, LondonVibhuti JainBelum ada peringkat
- SMC VM Eu PDFDokumen66 halamanSMC VM Eu PDFjoguvBelum ada peringkat