Anda mungkin juga menyukai
- Monograph of Qi ProjectDokumen29 halamanMonograph of Qi ProjectmerahiBelum ada peringkat
- Diagnosis, Evaluation, Prevention, and Treatment of CKD-MBDDokumen71 halamanDiagnosis, Evaluation, Prevention, and Treatment of CKD-MBDJinnasit Tee0% (1)
- Panduan Triage Revisi 2018Dokumen20 halamanPanduan Triage Revisi 2018Gery ApridoBelum ada peringkat
- Mukerji Committee Report 1966Dokumen47 halamanMukerji Committee Report 1966lalit823187100% (1)
- The Influence of Employee Engagement, Quality of Work Life and Organizational Commitment On Turnover Intention of Nurses From Grestelina Makassar Hospital in 2022Dokumen8 halamanThe Influence of Employee Engagement, Quality of Work Life and Organizational Commitment On Turnover Intention of Nurses From Grestelina Makassar Hospital in 2022Lawyer PaembonanBelum ada peringkat
- 4140 QI PosterDokumen1 halaman4140 QI PosterZoe RaineBelum ada peringkat
- Creating Service Concepts For Finnish Elderly Care: Promise NwaguDokumen95 halamanCreating Service Concepts For Finnish Elderly Care: Promise NwaguRichard HutasoitBelum ada peringkat
- Irene Diamond TKR Brochure-PrintDokumen39 halamanIrene Diamond TKR Brochure-PrintTusan Sidharta100% (1)
- Framework For HR ADokumen52 halamanFramework For HR AHS RattiBelum ada peringkat
- 1) Roles and Responsibilities of MLHPDokumen25 halaman1) Roles and Responsibilities of MLHPShankar MurariBelum ada peringkat
- Loyalitas PasienDokumen6 halamanLoyalitas PasienAnzzis Alfian PrabowoBelum ada peringkat
- ANA Nursing Sensitive Indicator PDFDokumen29 halamanANA Nursing Sensitive Indicator PDFAchmad Hidayatullah HafidBelum ada peringkat
- Mod2 - Ch3 - Health IndicatorsDokumen13 halamanMod2 - Ch3 - Health IndicatorsSara Sunabara100% (1)
- KERANGKA ACUAN KEGIATAN PROGRAM TB PARU. Tuberkulosis Adalah Penyaki Tmenular Langsung Yang Disebabkan Oleh Kuman PDFDokumen4 halamanKERANGKA ACUAN KEGIATAN PROGRAM TB PARU. Tuberkulosis Adalah Penyaki Tmenular Langsung Yang Disebabkan Oleh Kuman PDFAna UmulBelum ada peringkat
- Revisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesDokumen8 halamanRevisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesTiti Multi SaariBelum ada peringkat
- NCD Monthly Report April 2021 PAGE1Dokumen1 halamanNCD Monthly Report April 2021 PAGE1ekta priyawandanaBelum ada peringkat
- OIR23 - Digital ProgramDokumen7 halamanOIR23 - Digital ProgramU of T MedicineBelum ada peringkat
- Baju RakorDokumen32 halamanBaju RakorDPK Rumkit Bhayangkara Tk IBelum ada peringkat
- Apollo Master Health CheckDokumen2 halamanApollo Master Health ChecksreedevichBelum ada peringkat
- Analisis Pengendalian Potensi Fraud Di RDokumen7 halamanAnalisis Pengendalian Potensi Fraud Di RWahyudi KuncoroBelum ada peringkat
- DR, Junaid CV 2016Dokumen10 halamanDR, Junaid CV 2016Junaid NazarBelum ada peringkat
- Credentialing IsDokumen35 halamanCredentialing IsYetti DarmiBelum ada peringkat
- National Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesDokumen103 halamanNational Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesAdil AhmedBelum ada peringkat
- Proceeding 47th APACPH PDFDokumen650 halamanProceeding 47th APACPH PDFRosmawati DraBelum ada peringkat
- The Socio-Cultural Factors On Health and Illness - A StudyDokumen7 halamanThe Socio-Cultural Factors On Health and Illness - A StudyIJRASETPublicationsBelum ada peringkat
- National Cancer Control Programmes in ThailandDokumen93 halamanNational Cancer Control Programmes in ThailandIndonesian Journal of CancerBelum ada peringkat
- IHITool QIProjectMeasuresWorksheetDokumen3 halamanIHITool QIProjectMeasuresWorksheetDiah PutriBelum ada peringkat
- Poster PresentationDokumen1 halamanPoster Presentationapi-316009237Belum ada peringkat
- Final Supervision Checklist DocumentDokumen5 halamanFinal Supervision Checklist Documentotis2ke9588100% (1)
- Sop PdcaDokumen3 halamanSop PdcateemBelum ada peringkat
- Curriculum Vitae 2Dokumen3 halamanCurriculum Vitae 2kevin muchungaBelum ada peringkat
- JCI International Library of Measures ANIK BUKUDokumen325 halamanJCI International Library of Measures ANIK BUKUnurulBelum ada peringkat
- Malignant Pleural Effusion PrevalenceDokumen72 halamanMalignant Pleural Effusion PrevalenceAkbar SyarialBelum ada peringkat
- Epidemiology and Natural History Cervical CancerDokumen30 halamanEpidemiology and Natural History Cervical Cancermuhammadnurul asmiBelum ada peringkat
- 02 - Lifestyle and NCD - MEDF1120 - Prof. Martin WongDokumen48 halaman02 - Lifestyle and NCD - MEDF1120 - Prof. Martin WongdenisemywongBelum ada peringkat
- Managing Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoDokumen45 halamanManaging Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoaprinaaaBelum ada peringkat
- TB India 2017Dokumen173 halamanTB India 2017dratultiwariBelum ada peringkat
- Materi DrharrypDokumen38 halamanMateri DrharrypAnnisa Aisyha MalikBelum ada peringkat
- CCO Cytokine TX in MM ExpressPointsDokumen18 halamanCCO Cytokine TX in MM ExpressPointsveaceslav coscodanBelum ada peringkat
- Pediatric and Adult ECMO Patient Selection and ManagementDokumen58 halamanPediatric and Adult ECMO Patient Selection and ManagementPERFUZIJABelum ada peringkat
- Role of Finerenone As New Pillar in CKD Management in T2D Patients - GPMPDokumen29 halamanRole of Finerenone As New Pillar in CKD Management in T2D Patients - GPMPTaufiqurrokhman RofiiBelum ada peringkat
- Treat Cancer - CurrentDokumen49 halamanTreat Cancer - CurrentUzair Ul GhaniBelum ada peringkat
- Malaysia STI Guidelines 2015 PDFDokumen103 halamanMalaysia STI Guidelines 2015 PDFDerrick Ezra Ng100% (7)
- District PPM coordinators training agendaDokumen64 halamanDistrict PPM coordinators training agendaAbhijit DeyBelum ada peringkat
- Emerging Healthcare Technologies and The Future of Medicine: Ogan GurelDokumen22 halamanEmerging Healthcare Technologies and The Future of Medicine: Ogan GurelogangurelBelum ada peringkat
- 2021 Philippine Guidelines On PHEx Phase 1Dokumen148 halaman2021 Philippine Guidelines On PHEx Phase 1Famed residentsBelum ada peringkat
- Iaft 07 I 2 P 114Dokumen4 halamanIaft 07 I 2 P 114ashajangamBelum ada peringkat
- Awad 2016Dokumen8 halamanAwad 2016PopyBelum ada peringkat
- MNCR 2012-2016 Final (Published 2019) PDFDokumen116 halamanMNCR 2012-2016 Final (Published 2019) PDFWei Ying TanBelum ada peringkat
- CPG Dyslipidemia 2017 PPT SummaryDokumen25 halamanCPG Dyslipidemia 2017 PPT SummaryhakimahsBelum ada peringkat
- Medscape Emedicine: Specialty SitesDokumen4 halamanMedscape Emedicine: Specialty SitesEngelbert Carr BaldomanBelum ada peringkat
- Thromboembolic Disease During Tuberculosis: A Series of 47 CasesDokumen6 halamanThromboembolic Disease During Tuberculosis: A Series of 47 CasesIJAR JOURNALBelum ada peringkat
- Public Health Status and Challenges in NepalDokumen19 halamanPublic Health Status and Challenges in NepalSandip KumarBelum ada peringkat
- Development and Implementation of National NCD ProgrammeDokumen42 halamanDevelopment and Implementation of National NCD ProgrammeMadu JayathilakaBelum ada peringkat
- Posters & Handouts - CHODokumen56 halamanPosters & Handouts - CHODk YadavBelum ada peringkat
- Beneficial Effect of Cardiac Rehabilitation On Moroccan Patients After Valvular SurgeryDokumen5 halamanBeneficial Effect of Cardiac Rehabilitation On Moroccan Patients After Valvular SurgeryIJAR JOURNALBelum ada peringkat
- Final Breast Axillary and SCV Nodes Due Apr 24Dokumen27 halamanFinal Breast Axillary and SCV Nodes Due Apr 24api-569174359Belum ada peringkat
- Tumor Board - Mucinous.Dokumen54 halamanTumor Board - Mucinous.Apmc SchwartzBelum ada peringkat
- Cancer Burden in China Trends, Risk Factors and PreventionDokumen17 halamanCancer Burden in China Trends, Risk Factors and PreventioncursinhoprevestibBelum ada peringkat
- Medication Safety Workshop Final2Dokumen36 halamanMedication Safety Workshop Final2gHAZIBelum ada peringkat
- Why, What, How Green BuildingDokumen48 halamanWhy, What, How Green BuildingIndonesian Journal of CancerBelum ada peringkat
- Chemotherapy in Dharmais Cancer HospitalDokumen29 halamanChemotherapy in Dharmais Cancer HospitalIndonesian Journal of CancerBelum ada peringkat
- Cervical & Breast Cancer Screening ProgramDokumen22 halamanCervical & Breast Cancer Screening ProgramIndonesian Journal of CancerBelum ada peringkat
- Implementasi Konsep "Green Building" Pada Rumah SakitDokumen50 halamanImplementasi Konsep "Green Building" Pada Rumah SakitIndonesian Journal of Cancer100% (3)
- PACT A Partnership To Fight Cancer in Developing CountriesDokumen24 halamanPACT A Partnership To Fight Cancer in Developing CountriesIndonesian Journal of CancerBelum ada peringkat
- Supporting Cancer Management: Conceptual Framework TCMDokumen39 halamanSupporting Cancer Management: Conceptual Framework TCMIndonesian Journal of CancerBelum ada peringkat
- Production of Affordable ChemotherapyDokumen27 halamanProduction of Affordable ChemotherapyIndonesian Journal of CancerBelum ada peringkat
- Construction, Project ChecklistDokumen3 halamanConstruction, Project ChecklistIndonesian Journal of Cancer100% (2)
- Building Sustainable Cancer Control Capacity and Infrastructure in Developing CountriesDokumen25 halamanBuilding Sustainable Cancer Control Capacity and Infrastructure in Developing CountriesIndonesian Journal of CancerBelum ada peringkat
- New Advanced in RadiotherapyDokumen49 halamanNew Advanced in RadiotherapyIndonesian Journal of CancerBelum ada peringkat
- National Cancer Control Program in Indonesia, Role of Stake HolderDokumen12 halamanNational Cancer Control Program in Indonesia, Role of Stake HolderIndonesian Journal of CancerBelum ada peringkat
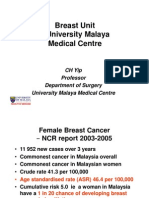
- Breast Unit - University Malaya Medical CentreDokumen47 halamanBreast Unit - University Malaya Medical CentreIndonesian Journal of CancerBelum ada peringkat
- Early Breast Cancer Detection Through Clinical Breast Examination Training For Midwives in Rural Jakarta, IndonesiaDokumen31 halamanEarly Breast Cancer Detection Through Clinical Breast Examination Training For Midwives in Rural Jakarta, IndonesiaIndonesian Journal of CancerBelum ada peringkat
- RS Onkologi Surabaya (Boutique Hospital Concept), An Alternative Model For Secondary CareDokumen49 halamanRS Onkologi Surabaya (Boutique Hospital Concept), An Alternative Model For Secondary CareIndonesian Journal of CancerBelum ada peringkat
- Dharmais National Cancer Center Indonesia, The Role in National Cancer Control Program of IndonesiaDokumen25 halamanDharmais National Cancer Center Indonesia, The Role in National Cancer Control Program of IndonesiaIndonesian Journal of Cancer100% (1)
- Enumeration of CD34+ Stem Cells Using FlowcytometryDokumen44 halamanEnumeration of CD34+ Stem Cells Using FlowcytometryIndonesian Journal of CancerBelum ada peringkat
- AffordableDokumen31 halamanAffordableIndonesian Journal of CancerBelum ada peringkat
- Role of Blood Bank in Stem Cells TherapyDokumen27 halamanRole of Blood Bank in Stem Cells TherapyIndonesian Journal of CancerBelum ada peringkat
- Bone Marrow and Umbilical Cord Blood TranplantationDokumen11 halamanBone Marrow and Umbilical Cord Blood TranplantationIndonesian Journal of CancerBelum ada peringkat
- Indonesia Cancer Registry, Current SituationDokumen68 halamanIndonesia Cancer Registry, Current SituationIndonesian Journal of Cancer100% (1)
- Bone Marrow TranplantationDokumen32 halamanBone Marrow TranplantationIndonesian Journal of CancerBelum ada peringkat
- Implementation of Cancer Control Programs, Cancer Prevention ResearchDokumen16 halamanImplementation of Cancer Control Programs, Cancer Prevention ResearchIndonesian Journal of CancerBelum ada peringkat
- Cancer Registry Data Quality and AnalysisDokumen42 halamanCancer Registry Data Quality and AnalysisIndonesian Journal of CancerBelum ada peringkat
- Research in Natural Product For Supporting Cancer ManagementDokumen44 halamanResearch in Natural Product For Supporting Cancer ManagementIndonesian Journal of Cancer100% (1)
- BINUS University: Bioinformatics Road MapDokumen16 halamanBINUS University: Bioinformatics Road MapIndonesian Journal of CancerBelum ada peringkat
- How To Increase Awareness in Cancer Through Healthy Lifestyle Empowerment in CommunityDokumen29 halamanHow To Increase Awareness in Cancer Through Healthy Lifestyle Empowerment in CommunityIndonesian Journal of CancerBelum ada peringkat
- Cancer Epidemiology and Program Implementation in Low and Middle Income (LMI) Countries: A Lesson To LearnDokumen56 halamanCancer Epidemiology and Program Implementation in Low and Middle Income (LMI) Countries: A Lesson To LearnIndonesian Journal of CancerBelum ada peringkat
- Role of BATAN in Establishing Nuclear Oncology in IndonesiaDokumen24 halamanRole of BATAN in Establishing Nuclear Oncology in IndonesiaIndonesian Journal of CancerBelum ada peringkat
- Status of Art of Cancer Center in EuropeDokumen35 halamanStatus of Art of Cancer Center in EuropeIndonesian Journal of CancerBelum ada peringkat
- Research Report WritingDokumen88 halamanResearch Report WritingIndonesian Journal of CancerBelum ada peringkat
- Fat in The Diet and Mortality From Heart Disease - Yerushalmy & HilleboeDokumen12 halamanFat in The Diet and Mortality From Heart Disease - Yerushalmy & HilleboeacolpoBelum ada peringkat
- Resettlement and Rehabilitation of People: Its Problems and ConcernsDokumen3 halamanResettlement and Rehabilitation of People: Its Problems and ConcernsGourabBelum ada peringkat
- (Donald J. Ortner) Human PaleopathologyDokumen328 halaman(Donald J. Ortner) Human Paleopathologymila_agBelum ada peringkat
- Application & Medical Forms Cir 2Dokumen2 halamanApplication & Medical Forms Cir 2Ivan FrancisBelum ada peringkat
- Lecture 1 - Introduction and History of EpiDokumen66 halamanLecture 1 - Introduction and History of Epivairakangal100% (1)
- Indigenous Traditional MedicineDokumen12 halamanIndigenous Traditional MedicinerathiasBelum ada peringkat
- Genomics Bioinformatics & Medicine Course SyllabusDokumen19 halamanGenomics Bioinformatics & Medicine Course SyllabusJohnny RodriguezBelum ada peringkat
- CHNN FNCP ScriptDokumen7 halamanCHNN FNCP ScriptArnel MacabalitaoBelum ada peringkat
- Executive Summary:: To Reach The Breakeven Point It Will Take Minimum of 8 Years (Approx.)Dokumen29 halamanExecutive Summary:: To Reach The Breakeven Point It Will Take Minimum of 8 Years (Approx.)sabrina akther eshaBelum ada peringkat
- Diagnosis and Treatment of The Disorders of PigsDokumen409 halamanDiagnosis and Treatment of The Disorders of PigsStevanBelum ada peringkat
- 10 - 1007 - 978 3 030 64869 5Dokumen119 halaman10 - 1007 - 978 3 030 64869 5Maria Grecu100% (1)
- A Seminar About History TakingDokumen13 halamanA Seminar About History Takingdr_jamal1983Belum ada peringkat
- Adapting To Major Chronic Illness A Proposal For ADokumen6 halamanAdapting To Major Chronic Illness A Proposal For ALaura RomeroBelum ada peringkat
- Factors Affecting Health and IllnessDokumen13 halamanFactors Affecting Health and IllnessEduard100% (4)
- RCI-CEL-AZA PEME FormA-Rev09-2019 FormB MedCertDokumen8 halamanRCI-CEL-AZA PEME FormA-Rev09-2019 FormB MedCertVhal AlbientoBelum ada peringkat
- Community Diagnosis FormatDokumen3 halamanCommunity Diagnosis FormatGen Franches Kyle ErigbuagasBelum ada peringkat
- Oswego Church Supper Gastrointestinal Outbreak Linked to Vanilla Ice CreamDokumen4 halamanOswego Church Supper Gastrointestinal Outbreak Linked to Vanilla Ice Creammidwestchic67% (3)
- Health TalkDokumen4 halamanHealth TalkAndalBelum ada peringkat
- Why Do We Fall Ill Lesson PlanDokumen7 halamanWhy Do We Fall Ill Lesson Planvijos16655Belum ada peringkat
- CAPE Biology Unit 2 ProjectDokumen13 halamanCAPE Biology Unit 2 ProjectAudi Sweetangel0% (1)
- Pathogens: A 2021 Update On Syphilis: Taking Stock From Pathogenesis To VaccinesDokumen14 halamanPathogens: A 2021 Update On Syphilis: Taking Stock From Pathogenesis To Vaccinesgupro tahiBelum ada peringkat
- DC 2020-0106 Use of WHO Interim Guidleines For Health Workers Exposure Risk Assessemnt and Mangement in The Context of COVID-19 VirusDokumen9 halamanDC 2020-0106 Use of WHO Interim Guidleines For Health Workers Exposure Risk Assessemnt and Mangement in The Context of COVID-19 VirusJoselito P. PlatillaBelum ada peringkat
- WHO HSE GCR 2015.5 Eng PDFDokumen180 halamanWHO HSE GCR 2015.5 Eng PDFFull ColourBelum ada peringkat
- Amenuvi MDokumen2 halamanAmenuvi MMawulorm AmenuvieBelum ada peringkat
- HIV and AIDS explainedDokumen1 halamanHIV and AIDS explainedKevinBelum ada peringkat
- Diabetes Book THAI-ENGDokumen100 halamanDiabetes Book THAI-ENGNaharuthai BumrungratanayosBelum ada peringkat
- 000-Intro To Internal MedicineDokumen6 halaman000-Intro To Internal MedicineRizky KykyBelum ada peringkat
- WEEK 1 - OVERVIEW OF HEALTH ASSESSMENTDokumen4 halamanWEEK 1 - OVERVIEW OF HEALTH ASSESSMENTDharyn KhaiBelum ada peringkat
- Baguio Central University College of Nursing Comprehensive Exam.-ChnDokumen9 halamanBaguio Central University College of Nursing Comprehensive Exam.-ChnKristian Karl Bautista Kiw-isBelum ada peringkat
- Certificate of Health SummaryDokumen2 halamanCertificate of Health SummaryNK productionBelum ada peringkat