Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- On How To Design A Low Voltage SwitchboardDokumen11 halamanOn How To Design A Low Voltage SwitchboardsabeerBelum ada peringkat
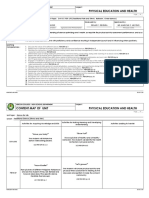
- Content Map PE & Health 12Dokumen12 halamanContent Map PE & Health 12RIZZA MEA DOLOSOBelum ada peringkat
- DAMPNESSDokumen21 halamanDAMPNESSChukwu SolomonBelum ada peringkat
- RIASEC Personality TestDokumen2 halamanRIASEC Personality TestSarah Jane NomoBelum ada peringkat
- Shoulder Joint Position Sense Improves With ElevationDokumen10 halamanShoulder Joint Position Sense Improves With ElevationpredragbozicBelum ada peringkat
- Factors That Contribute To Successful BakingDokumen8 halamanFactors That Contribute To Successful BakingErrol San Juan100% (1)
- Toxic RelationshipDokumen1 halamanToxic RelationshipwidyasBelum ada peringkat
- Planificare Săptămânală - Clasa A II-a (Fairyland 2)Dokumen6 halamanPlanificare Săptămânală - Clasa A II-a (Fairyland 2)Oxy Oxy100% (1)
- PBL 2 Case PresentationDokumen12 halamanPBL 2 Case PresentationRamish IrfanBelum ada peringkat
- Pearls and Pitfalls in Emergency Radiology Variants and Other Difficult Diagnoses 2013Dokumen389 halamanPearls and Pitfalls in Emergency Radiology Variants and Other Difficult Diagnoses 2013mmbire@gmail.comBelum ada peringkat
- Hema Lec HematopoiesisDokumen8 halamanHema Lec HematopoiesisWayne ErumaBelum ada peringkat
- Demolition/Removal Permit Application Form: Planning, Property and Development DepartmentDokumen3 halamanDemolition/Removal Permit Application Form: Planning, Property and Development DepartmentAl7amdlellahBelum ada peringkat
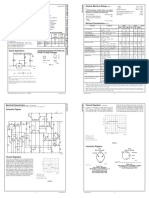
- LM 337Dokumen4 halamanLM 337matias robertBelum ada peringkat
- Celltac MEK 6500Dokumen3 halamanCelltac MEK 6500RiduanBelum ada peringkat
- Defects Lamellar TearingDokumen6 halamanDefects Lamellar Tearingguru_terexBelum ada peringkat
- Intimacy and Healthy Affective Maturaity - Fa-Winter09bDokumen9 halamanIntimacy and Healthy Affective Maturaity - Fa-Winter09bCarlos GiraldoBelum ada peringkat
- Critical Care Nursing Assessment Form: R R R R R R R RDokumen2 halamanCritical Care Nursing Assessment Form: R R R R R R R RPipit Permata100% (1)
- DET Tronics: Unitized UV/IR Flame Detector U7652Dokumen2 halamanDET Tronics: Unitized UV/IR Flame Detector U7652Julio Andres Garcia PabolaBelum ada peringkat
- W4. Grade 10 Health - Q1 - M4 - v2Dokumen22 halamanW4. Grade 10 Health - Q1 - M4 - v2Jesmael PantalunanBelum ada peringkat
- PMA 2015 2016 Issue 3 PDFDokumen36 halamanPMA 2015 2016 Issue 3 PDFLyndon Mercado TolentinoBelum ada peringkat
- Injection Analyzer Electronic Unit enDokumen67 halamanInjection Analyzer Electronic Unit enmayralizbethbustosBelum ada peringkat
- Preservative MaterialsDokumen2 halamanPreservative MaterialsmtcengineeringBelum ada peringkat
- Do Statins Lower TestosteroneDokumen3 halamanDo Statins Lower TestosteroneNandia SeptiyoriniBelum ada peringkat
- TCM Reach TrucksDokumen5 halamanTCM Reach TrucksMuhammad SohailBelum ada peringkat
- J. Bleger ArtDokumen10 halamanJ. Bleger Artivancristina42Belum ada peringkat
- Course Weekly Schedule Health Science TheoryDokumen6 halamanCourse Weekly Schedule Health Science Theoryapi-466810096Belum ada peringkat
- 3 14 Revision Guide Organic SynthesisDokumen6 halaman3 14 Revision Guide Organic SynthesisCin D NgBelum ada peringkat
- Boli Vertebro MedulareDokumen12 halamanBoli Vertebro MedulareHalit DianaBelum ada peringkat
- Leave of Absence Form (Rev. 02 072017)Dokumen1 halamanLeave of Absence Form (Rev. 02 072017)KIMBERLY BALISACANBelum ada peringkat
- Nephrotic SyndromeDokumen56 halamanNephrotic SyndromeMurugesan100% (1)