Anda mungkin juga menyukai
- ScoliosisDokumen25 halamanScoliosisshanel18100% (1)
- TractionDokumen79 halamanTractionKoRnflakes100% (9)
- Herniated Nucleus PulposusDokumen14 halamanHerniated Nucleus PulposusJm Fernandez Gan RNBelum ada peringkat
- 5.casts and MoldsDokumen30 halaman5.casts and MoldsKatrina PonceBelum ada peringkat
- Benign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFDokumen8 halamanBenign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFegyzellahsBelum ada peringkat
- Process RecordingDokumen12 halamanProcess RecordingIanna J. L. PedrosaBelum ada peringkat
- University of Northern PhilippinesDokumen30 halamanUniversity of Northern PhilippinesClaudine JaramilloBelum ada peringkat
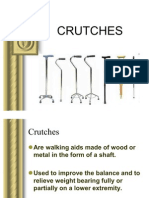
- CRUTCHESDokumen35 halamanCRUTCHESBebing CostinianoBelum ada peringkat
- Scoliosis MedbackDokumen18 halamanScoliosis MedbackVanessa Yvonne GurtizaBelum ada peringkat
- Surgical Instruments 1x1Dokumen9 halamanSurgical Instruments 1x1Nikael Patun-ogBelum ada peringkat
- Circular Railway Revival Project - Signaling PDFDokumen151 halamanCircular Railway Revival Project - Signaling PDFpoketupiBelum ada peringkat
- Prepared By:: Ma. Kristina G. CristobalDokumen17 halamanPrepared By:: Ma. Kristina G. CristobalDiovy TahilanBelum ada peringkat
- Traction NewDokumen37 halamanTraction Newapi-3716867100% (1)
- Compartment Syndrome: Return To TopDokumen3 halamanCompartment Syndrome: Return To TopSania Kamal BalweelBelum ada peringkat
- Cast and MoldsDokumen3 halamanCast and MoldsKimberlee Ced Garcia NoolBelum ada peringkat
- Elbow TraumaDokumen62 halamanElbow Traumadrcoolcat2000Belum ada peringkat
- Anatomy of ScoliosisDokumen6 halamanAnatomy of ScoliosisDaniel MañalacBelum ada peringkat
- Cast and TractionsDokumen12 halamanCast and TractionsNoemi Nazareno MarceloBelum ada peringkat
- Basic Orthopedic HardwareDokumen13 halamanBasic Orthopedic HardwareJennifer C. SumadsadBelum ada peringkat
- Anatomy and PhysiologyDokumen4 halamanAnatomy and PhysiologyAnnileighjeanBelum ada peringkat
- Femoral Neck FractureDokumen36 halamanFemoral Neck FractureAnonymous ekem7I100% (2)
- SURGERY - Basic Surgical InstrumentsDokumen19 halamanSURGERY - Basic Surgical InstrumentsMaie CabanagBelum ada peringkat
- Cast and BracesDokumen6 halamanCast and BracesCazxie DumlaoBelum ada peringkat
- POC Review NotesDokumen9 halamanPOC Review NotesMagdaraog Gabrielle A.Belum ada peringkat
- Skeletal TractionDokumen7 halamanSkeletal TractionAnnalyn Austria100% (2)
- Operating Room Instruments by JheaaDokumen78 halamanOperating Room Instruments by JheaaSareno PJhēa100% (1)
- Femoral Neck FracturesDokumen10 halamanFemoral Neck FracturesMorshed Mahbub AbirBelum ada peringkat
- Common or InstrumentsDokumen16 halamanCommon or InstrumentsCosmic PhilippinesBelum ada peringkat
- POC - Review NotesDokumen9 halamanPOC - Review NotesSTEFFI GABRIELLE GOLEZBelum ada peringkat
- Application Balanced Skeletal TractionDokumen6 halamanApplication Balanced Skeletal TractionLorenz ChristopherBelum ada peringkat
- Clavicle FractureDokumen4 halamanClavicle FracturesridharBelum ada peringkat
- Orthopedic NursingDokumen2 halamanOrthopedic NursingMichelle TamorBelum ada peringkat
- Orthopedic Problem and ManagementDokumen42 halamanOrthopedic Problem and Managementjosephabram051590Belum ada peringkat
- Pott Disease 1223292121651385 8Dokumen54 halamanPott Disease 1223292121651385 8Ismail SalimBelum ada peringkat
- The Balanced Skeletal TractionDokumen1 halamanThe Balanced Skeletal TractionGemarie Adarlo CastilloBelum ada peringkat
- Hardware Ortho.Dokumen35 halamanHardware Ortho.karendelarosa06277100% (2)
- Medical Glossary Midterms ExamDokumen7 halamanMedical Glossary Midterms ExamFev BanataoBelum ada peringkat
- Common Surgical Instruments ModuleDokumen5 halamanCommon Surgical Instruments ModuleAlokKumarBelum ada peringkat
- Handout Orthopedic Nursing Assisstive DevicesDokumen14 halamanHandout Orthopedic Nursing Assisstive DevicesPaul Christian P. Santos, RN100% (2)
- La Consolacion College Manila: Femoral Neck FractureDokumen3 halamanLa Consolacion College Manila: Femoral Neck FractureIvan Liquiran AvenadoBelum ada peringkat
- Predisposing Factors: Independent:: Assessment Cues Nursing Diagnosis Schematic Diagram Rationale EvaluationDokumen2 halamanPredisposing Factors: Independent:: Assessment Cues Nursing Diagnosis Schematic Diagram Rationale EvaluationCarla Tongson MaravillaBelum ada peringkat
- Amoebiasis Case StudyDokumen13 halamanAmoebiasis Case StudymelvinpasionaBelum ada peringkat
- Communicable Disease NursingDokumen16 halamanCommunicable Disease NursingWawit A Dela CernaBelum ada peringkat
- Cast and Splint Immobilization - Complications PDFDokumen11 halamanCast and Splint Immobilization - Complications PDFcronoss21Belum ada peringkat
- 668-Osgood-Schlatter Powerpoint Spring 2015Dokumen38 halaman668-Osgood-Schlatter Powerpoint Spring 2015api-280210660Belum ada peringkat
- Anthropometric Measurements 2Dokumen19 halamanAnthropometric Measurements 2Gajender SharmaBelum ada peringkat
- FNCPDokumen5 halamanFNCPCindy MariscotesBelum ada peringkat
- Splints and Casts Indications and MethodsDokumen9 halamanSplints and Casts Indications and MethodsJay GaneshBelum ada peringkat
- CastDokumen16 halamanCastSheena Flores Abuga-a100% (1)
- Potts DiseaseDokumen8 halamanPotts Diseaseaimeeros0% (2)
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDokumen4 halamanSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaBelum ada peringkat
- Case Study: Fracture, Open III A, Compound Comminuted Distal 3 Tibia, LeftDokumen19 halamanCase Study: Fracture, Open III A, Compound Comminuted Distal 3 Tibia, LeftmarzcuteBelum ada peringkat
- Fracture ManagementDokumen19 halamanFracture ManagementManaha Sekonyela TjamelaBelum ada peringkat
- Molds and Orthopedic HardwareDokumen33 halamanMolds and Orthopedic HardwareyelbonifacioBelum ada peringkat
- Ingrown Toenail (Onychocryptosis)Dokumen18 halamanIngrown Toenail (Onychocryptosis)Ray Yankees100% (1)
- Medical Surgical Nursing Module 14Dokumen31 halamanMedical Surgical Nursing Module 14weissBelum ada peringkat
- Types of WoundsDokumen2 halamanTypes of WoundsMike Luther ManingoBelum ada peringkat
- Osteomyelitis PDFDokumen39 halamanOsteomyelitis PDFxxsaptxxBelum ada peringkat
- Ortho BracesDokumen6 halamanOrtho BracesSanny RamosBelum ada peringkat
- Fractures, PathophysiologyDokumen1 halamanFractures, Pathophysiology4kscribdBelum ada peringkat
- Close Right Arm Fracture: Our Lady of Fatima University College of NursingDokumen12 halamanClose Right Arm Fracture: Our Lady of Fatima University College of NursingBrylle Capili100% (1)
- 08 BQ - PADSB - Elect - P2 - R2 (Subcon Empty BQ)Dokumen89 halaman08 BQ - PADSB - Elect - P2 - R2 (Subcon Empty BQ)Middle EastBelum ada peringkat
- Barclays Personal Savings AccountsDokumen10 halamanBarclays Personal Savings AccountsTHBelum ada peringkat
- Factors Influencing The Selection Of: MaterialsDokumen22 halamanFactors Influencing The Selection Of: MaterialsMaulik KotadiyaBelum ada peringkat
- Graph 1: Temperature,° C of Mixture 1 (Naoh-Hcl) Against Time Taken, (Min)Dokumen8 halamanGraph 1: Temperature,° C of Mixture 1 (Naoh-Hcl) Against Time Taken, (Min)LeeshaaLenee Paramanantha KumarBelum ada peringkat
- Zencrack Installation and ExecutionDokumen48 halamanZencrack Installation and ExecutionJu waBelum ada peringkat
- Basic Customer Service SkillsDokumen90 halamanBasic Customer Service SkillsGillian Delos ReyesBelum ada peringkat
- Bharat Sanchar Nigam Limited: Invoice For Post Paid ServicesDokumen2 halamanBharat Sanchar Nigam Limited: Invoice For Post Paid ServicessuryaBelum ada peringkat
- Train Collision Avoidance SystemDokumen4 halamanTrain Collision Avoidance SystemSaurabh GuptaBelum ada peringkat
- Libra Office Question Answer EnglishDokumen11 halamanLibra Office Question Answer EnglishAndrew ParkarBelum ada peringkat
- Request Please Only Students Who Are Willing To Join in Haryana in Any District Are Requested To Apply For JobDokumen2 halamanRequest Please Only Students Who Are Willing To Join in Haryana in Any District Are Requested To Apply For JobUdayan KarnatakBelum ada peringkat
- Model-Checking: A Tutorial Introduction: January 1999Dokumen26 halamanModel-Checking: A Tutorial Introduction: January 1999Quý Trương QuangBelum ada peringkat
- JapanDokumen15 halamanJapanceazar BugtongBelum ada peringkat
- BE 503 - Week 1 - Analysis 7.18.11Dokumen6 halamanBE 503 - Week 1 - Analysis 7.18.11dwoodburyBelum ada peringkat
- Marketing Plan Potato Food TruckDokumen25 halamanMarketing Plan Potato Food TruckAhasan h. ShuvoBelum ada peringkat
- Freedom SW 2000 Owners Guide (975-0528!01!01 - Rev-D)Dokumen48 halamanFreedom SW 2000 Owners Guide (975-0528!01!01 - Rev-D)MatthewBelum ada peringkat
- RK3066 Mid PDFDokumen17 halamanRK3066 Mid PDFSharon MurphyBelum ada peringkat
- Netflix Annual Report 2010Dokumen76 halamanNetflix Annual Report 2010Arman AliBelum ada peringkat
- Adherence Tradeoff To Multiple Preventive Therapies and All-Cause Mortality After Acute Myocardial InfarctionDokumen12 halamanAdherence Tradeoff To Multiple Preventive Therapies and All-Cause Mortality After Acute Myocardial InfarctionRoberto López MataBelum ada peringkat
- Microsoft 365 LicensingDokumen18 halamanMicrosoft 365 Licensingwendy yohanesBelum ada peringkat
- 1353apni KakshaDokumen43 halaman1353apni KakshaArush GautamBelum ada peringkat
- 2018-2021 VUMC Nursing Strategic Plan: Vision Core ValuesDokumen1 halaman2018-2021 VUMC Nursing Strategic Plan: Vision Core ValuesAmeng GosimBelum ada peringkat
- Problem Sheet 3 - External Forced Convection - WatermarkDokumen2 halamanProblem Sheet 3 - External Forced Convection - WatermarkUzair KhanBelum ada peringkat
- Airline and Airport Master - OdsDokumen333 halamanAirline and Airport Master - OdsGiri KumarBelum ada peringkat
- B. Tech. - CSE - R13-Syllabus JntuaDokumen132 halamanB. Tech. - CSE - R13-Syllabus JntuaVasim AkramBelum ada peringkat
- Research Topics For Economics Thesis in PakistanDokumen7 halamanResearch Topics For Economics Thesis in PakistanStacy Vasquez100% (2)
- Unit One Mathematical EconomicsDokumen15 halamanUnit One Mathematical EconomicsSitra AbduBelum ada peringkat
- Maruti FinalDokumen23 halamanMaruti FinalYash MangeBelum ada peringkat
- Vibration Absorbers: Scan This QR CodeDokumen4 halamanVibration Absorbers: Scan This QR CodeMohamed RaafatBelum ada peringkat
- Concept of InsuranceDokumen4 halamanConcept of InsuranceNazrul HoqueBelum ada peringkat