Anda mungkin juga menyukai
- Screening For MRSA by Dr.T.V.Rao MDDokumen30 halamanScreening For MRSA by Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- Artificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDDokumen34 halamanArtificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- Influenza Teaching Current Update 2023 by Dr.T.V.Rao MDDokumen100 halamanInfluenza Teaching Current Update 2023 by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- GRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDDokumen2 halamanGRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- Need For Clinical Microbiologists by Dr.T.V.Rao MDDokumen2 halamanNeed For Clinical Microbiologists by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- Surgical Operation Theater StandardsDokumen31 halamanSurgical Operation Theater Standardstummalapalli venkateswara raoBelum ada peringkat
- MDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDDokumen2 halamanMDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- INFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDDokumen25 halamanINFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- Who Is Killing Modern Medicine in IndiaDokumen3 halamanWho Is Killing Modern Medicine in Indiatummalapalli venkateswara raoBelum ada peringkat
- MALDI-ToF in Clinical MicrobiologyDokumen39 halamanMALDI-ToF in Clinical Microbiologytummalapalli venkateswara rao100% (1)
- MDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDDokumen33 halamanMDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDokumen28 halamanElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- Infection Control in Burns PatietnsDokumen41 halamanInfection Control in Burns Patietnstummalapalli venkateswara raoBelum ada peringkat
- Health Care Associated Infections Creating Drug Resistance AtlasDokumen46 halamanHealth Care Associated Infections Creating Drug Resistance Atlastummalapalli venkateswara raoBelum ada peringkat
- Auditing Hospital Associated InfectionsDokumen59 halamanAuditing Hospital Associated Infectionstummalapalli venkateswara raoBelum ada peringkat
- AUDITING ANTIBIOGRAMS by Dr.T.V.RaoMDDokumen55 halamanAUDITING ANTIBIOGRAMS by Dr.T.V.RaoMDtummalapalli venkateswara rao100% (1)
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDokumen61 halamanHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- MDR-TB An Update by Dr.T.V.Rao MDDokumen43 halamanMDR-TB An Update by Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- ZIKA VIRUS INFECTION Emerging Public Health ConcernDokumen36 halamanZIKA VIRUS INFECTION Emerging Public Health Concerntummalapalli venkateswara rao100% (1)
- INFECTIONS IN DIALYSIS PATIENTS Basis & Prevention by Dr.T.V.Rao MDDokumen48 halamanINFECTIONS IN DIALYSIS PATIENTS Basis & Prevention by Dr.T.V.Rao MDtummalapalli venkateswara raoBelum ada peringkat
- Revisiting Blood CulturingDokumen2 halamanRevisiting Blood Culturingtummalapalli venkateswara raoBelum ada peringkat
- Surgical Gloves in Health CareDokumen29 halamanSurgical Gloves in Health Caretummalapalli venkateswara raoBelum ada peringkat
- Medical Microbiology in Crisis in IndiaDokumen4 halamanMedical Microbiology in Crisis in Indiatummalapalli venkateswara raoBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Egg Allergy: Other Food Allergies in Children With An Egg AllergyDokumen4 halamanEgg Allergy: Other Food Allergies in Children With An Egg AllergySuthanthirapalan GowrishankarBelum ada peringkat
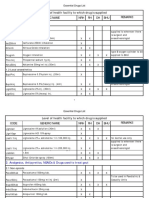
- Code Generic Name NRH RH DH BHU Remarks Level of Health Facility To Which Drug Is SuppliedDokumen42 halamanCode Generic Name NRH RH DH BHU Remarks Level of Health Facility To Which Drug Is SuppliedTob JurBelum ada peringkat
- Communicable Diseases ReviewerDokumen12 halamanCommunicable Diseases ReviewerEmy TandinganBelum ada peringkat
- Improved Chicken RearingDokumen4 halamanImproved Chicken RearingAnonymous asCQ7N7GVBelum ada peringkat
- Vaccinepeerreview PDFDokumen1.053 halamanVaccinepeerreview PDFMatthew SharpBelum ada peringkat
- NASYTA DIFA FIRDAUS - Tabel Pengelompokkan AntibiotikDokumen1 halamanNASYTA DIFA FIRDAUS - Tabel Pengelompokkan AntibiotikNasyta Difa FirdausBelum ada peringkat
- Organic NZ May 01 2018Dokumen68 halamanOrganic NZ May 01 2018Salva GarcíaBelum ada peringkat
- Interpretation of Hepatitis B Serologic Test ResultsDokumen1 halamanInterpretation of Hepatitis B Serologic Test ResultsarjumandBelum ada peringkat
- World Health Awareness DaysDokumen4 halamanWorld Health Awareness Daysbnrajeeva3344Belum ada peringkat
- Frequences RifeDokumen294 halamanFrequences Rifedoggydog100% (5)
- Referat Bronkopneumonia JulDokumen18 halamanReferat Bronkopneumonia Juljuliand hidayat100% (1)
- CHAPTER 1 - DraftDokumen16 halamanCHAPTER 1 - DraftARZELIE MARIE R. TOMBOCBelum ada peringkat
- Cap Guidelines 2010Dokumen42 halamanCap Guidelines 2010Marion Andrea PoblacionBelum ada peringkat
- D.S.S Aiims Prepration Test SeriesDokumen6 halamanD.S.S Aiims Prepration Test SeriesDr-Sanjay SinghaniaBelum ada peringkat
- Maklumat Vaksinasi: Vaccination DetailsDokumen2 halamanMaklumat Vaksinasi: Vaccination Detailsahmad hussainiBelum ada peringkat
- Biliary AtresiaDokumen9 halamanBiliary AtresiaPrabhakar KumarBelum ada peringkat
- Complete List of Vaccines 2016Dokumen8 halamanComplete List of Vaccines 2016Evangelist Michelle Leavy-BreunigBelum ada peringkat
- Rheumatic Heart DiseaseDokumen4 halamanRheumatic Heart DiseaseJhen Jhen100% (1)
- Lipofectamine ManualDokumen4 halamanLipofectamine ManualBui Ngoc ThuyBelum ada peringkat
- Kernow LMC Newsletter - August 2019 Edition FINAL USEDokumen15 halamanKernow LMC Newsletter - August 2019 Edition FINAL USECornwall and Isles of Scilly LMCBelum ada peringkat
- Antibiotic CMU 2557 ORC Shared View PDFDokumen60 halamanAntibiotic CMU 2557 ORC Shared View PDFSitthikorn StrikerrBelum ada peringkat
- Everything After VISADokumen20 halamanEverything After VISAvibhatiBelum ada peringkat
- Owners ManualDokumen115 halamanOwners ManualBurntToastBelum ada peringkat
- Allergic Rhinitis Diagnostic EvaluationDokumen2 halamanAllergic Rhinitis Diagnostic EvaluationDengz MendozaBelum ada peringkat
- Kernig Sign, Brudzinski Sign and Nuchal Rigidity By: PutrialishajsgDokumen24 halamanKernig Sign, Brudzinski Sign and Nuchal Rigidity By: Putrialishajsgfarah fadzilBelum ada peringkat
- Workshop ReportDokumen42 halamanWorkshop ReportSushila PaudelBelum ada peringkat
- UPDATES ON REPORT ON THE STATUS OF COVID-19 VACCINATION OF STA. MARIA NHS - 12 - 3 - 2021 (Responses)Dokumen19 halamanUPDATES ON REPORT ON THE STATUS OF COVID-19 VACCINATION OF STA. MARIA NHS - 12 - 3 - 2021 (Responses)Ben T OngBelum ada peringkat
- Communicable Diseases Causes, Control and Prevention Among Pre-School Age ChildrenDokumen4 halamanCommunicable Diseases Causes, Control and Prevention Among Pre-School Age ChildrenVinayagam VenkatesanBelum ada peringkat
- RH Blood Group System: Dr. Naveed MunirDokumen49 halamanRH Blood Group System: Dr. Naveed MuniriqrarBelum ada peringkat
- 3637 Technical Bulletin MTD Isa 760 vg4536718630311562122Dokumen1 halaman3637 Technical Bulletin MTD Isa 760 vg4536718630311562122Thảo ThảoBelum ada peringkat