Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Maternal Newborn Case Study Approach ToquestionsDokumen83 halamanMaternal Newborn Case Study Approach ToquestionsVin Lorenzo Campbell67% (6)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Fluid and Electrolytes Study GuideDokumen16 halamanFluid and Electrolytes Study GuideDianaNursing96% (28)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Snake Bite Ppt-1Dokumen53 halamanSnake Bite Ppt-1Arjit Bhushan100% (1)
- Safe Injection and Infusion PracticesDokumen32 halamanSafe Injection and Infusion Practicesniraj_sd75% (4)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Septic ShockDokumen18 halamanSeptic Shockshini sebastianBelum ada peringkat
- Soft Tissue SarcomasDokumen37 halamanSoft Tissue SarcomasHealth Education Library for People100% (1)
- RadiotherapyDokumen32 halamanRadiotherapyHealth Education Library for People100% (1)
- Stomach CancerDokumen29 halamanStomach CancerHealth Education Library for PeopleBelum ada peringkat
- Testicular CancerDokumen32 halamanTesticular CancerHealth Education Library for PeopleBelum ada peringkat
- Skin CancerDokumen27 halamanSkin CancerHealth Education Library for People100% (1)
- Stem Cell and Bone Marrow TransplantsDokumen20 halamanStem Cell and Bone Marrow TransplantsHealth Education Library for PeopleBelum ada peringkat
- Seondary Bone CancerDokumen24 halamanSeondary Bone CancerHealth Education Library for PeopleBelum ada peringkat
- Prostate CancerDokumen70 halamanProstate CancerHealth Education Library for People0% (1)
- Sexuality and CancerDokumen25 halamanSexuality and CancerHealth Education Library for PeopleBelum ada peringkat
- Pancreatic CancerDokumen30 halamanPancreatic CancerHealth Education Library for People75% (4)
- Non-Hodgkin LymphomaDokumen29 halamanNon-Hodgkin LymphomaHealth Education Library for People50% (2)
- Kidney CancerDokumen24 halamanKidney CancerHealth Education Library for PeopleBelum ada peringkat
- Ovarian CancerDokumen34 halamanOvarian CancerHealth Education Library for People100% (4)
- Malignant MelanomaDokumen29 halamanMalignant MelanomaHealth Education Library for People100% (2)
- LymphoedemaDokumen26 halamanLymphoedemaHealth Education Library for PeopleBelum ada peringkat
- Primary Bone CancerDokumen41 halamanPrimary Bone CancerHealth Education Library for PeopleBelum ada peringkat
- MyelomaDokumen32 halamanMyelomaHealth Education Library for PeopleBelum ada peringkat
- Liver CancerDokumen28 halamanLiver CancerHealth Education Library for PeopleBelum ada peringkat
- Lung CancerDokumen52 halamanLung CancerHealth Education Library for People50% (4)
- Head and Neck CancersDokumen50 halamanHead and Neck CancersHealth Education Library for PeopleBelum ada peringkat
- Hodgkins LymphomaDokumen26 halamanHodgkins LymphomaHealth Education Library for PeopleBelum ada peringkat
- Kaposi's SarcomaDokumen16 halamanKaposi's SarcomaHealth Education Library for People100% (1)
- Colon and Rectal CancerDokumen71 halamanColon and Rectal CancerHealth Education Library for People100% (1)
- Diet and The Cancer PatientDokumen23 halamanDiet and The Cancer PatientHealth Education Library for People100% (1)
- ChemotherapyDokumen30 halamanChemotherapyHealth Education Library for People100% (3)
- Chronic Myelogeneous LeukaemiaDokumen37 halamanChronic Myelogeneous LeukaemiaHealth Education Library for PeopleBelum ada peringkat
- Cancer of The VulvaDokumen24 halamanCancer of The VulvaHealth Education Library for PeopleBelum ada peringkat
- Cervical Screening & Cervical CancerDokumen53 halamanCervical Screening & Cervical CancerHealth Education Library for PeopleBelum ada peringkat
- Cancer of The Womb (Uterus)Dokumen20 halamanCancer of The Womb (Uterus)Health Education Library for PeopleBelum ada peringkat
- Drugs Interaction1Dokumen13 halamanDrugs Interaction1Akshay MandhotraBelum ada peringkat
- MUPAS, Grace Geraldine R. - Drug StudyDokumen17 halamanMUPAS, Grace Geraldine R. - Drug StudyGrace Geraldine MupasBelum ada peringkat
- Home Dialysis Nurse ResumeDokumen1 halamanHome Dialysis Nurse ResumeSiti FauziyahBelum ada peringkat
- Case Study On Anemia PDFDokumen33 halamanCase Study On Anemia PDFDrPreeti Thakur ChouhanBelum ada peringkat
- Operating Room EquipmentDokumen9 halamanOperating Room EquipmentgatordawgBelum ada peringkat
- Alaris Asena CC - User ManualDokumen21 halamanAlaris Asena CC - User Manualsmurd112100% (1)
- Nicardipine (Cardene ®) - Intravenous (IV) Dilution PDFDokumen3 halamanNicardipine (Cardene ®) - Intravenous (IV) Dilution PDFNovianWibowoDokterBelum ada peringkat
- Central ObjectiveDokumen20 halamanCentral ObjectiveValarmathiBelum ada peringkat
- IV Manual 7th Edition July 2020Dokumen175 halamanIV Manual 7th Edition July 2020Deena AlJawamisBelum ada peringkat
- Ralph's ProposalDokumen15 halamanRalph's ProposalHeilene Ethel AngcayaBelum ada peringkat
- Ailyn - Perez - ResumeDokumen6 halamanAilyn - Perez - ResumeJhullian Frederick Val VergaraBelum ada peringkat
- Standards of Medical Care in Diabetes-2022Dokumen10 halamanStandards of Medical Care in Diabetes-2022Adina SimionBelum ada peringkat
- The Many Benefits of Hydrogen PeroxideDokumen9 halamanThe Many Benefits of Hydrogen PeroxideRedza100% (7)
- Medication Calculations 2Dokumen26 halamanMedication Calculations 2loglesb1100% (2)
- Glypressin Serbuk Injeksi 1 Mg+pelarut - Terlipressin Asetat - DKI1951700144A1 - 2019Dokumen8 halamanGlypressin Serbuk Injeksi 1 Mg+pelarut - Terlipressin Asetat - DKI1951700144A1 - 2019edo adimastaBelum ada peringkat
- ENGLISH 3 WonogiriDokumen49 halamanENGLISH 3 WonogiriDewi HastutiBelum ada peringkat
- Onco Case StudyDokumen2 halamanOnco Case StudyAllenBelum ada peringkat
- Zimmer Traction Handbook PDFDokumen92 halamanZimmer Traction Handbook PDFMarilyn100% (1)
- 2022-Brochure Neonatal PiccDokumen4 halaman2022-Brochure Neonatal PiccNAIYA BHAVSARBelum ada peringkat
- Catheter Complication: Managing Pitfalls in IV Therapy: Perawat Hebat - Perawat TangguhDokumen37 halamanCatheter Complication: Managing Pitfalls in IV Therapy: Perawat Hebat - Perawat TangguhAdi SullivanBelum ada peringkat
- Shape Up - Prescription Labels Printing at PharmacyDokumen12 halamanShape Up - Prescription Labels Printing at PharmacyJulio AlemánBelum ada peringkat
- THROMBOPHLEBITISDokumen50 halamanTHROMBOPHLEBITISmers puno100% (3)
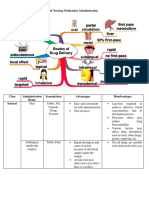
- Different Routes of Nursing Medication AdministrationDokumen13 halamanDifferent Routes of Nursing Medication AdministrationRonica MendozaBelum ada peringkat
- E Catalogue 2opDokumen196 halamanE Catalogue 2opChris-Goldie LorezoBelum ada peringkat
- Anatomy Physiology of Human BodyDokumen90 halamanAnatomy Physiology of Human BodyJesica ElviraBelum ada peringkat