Anda mungkin juga menyukai
- Game-Based Cognitive-Behavioral Therapy (GB-CBT) LEER PDFDokumen7 halamanGame-Based Cognitive-Behavioral Therapy (GB-CBT) LEER PDFkarenBelum ada peringkat
- Liver Function TestsDokumen3 halamanLiver Function TestsdanielazimzadehBelum ada peringkat
- Mental Status ExamDokumen10 halamanMental Status ExamSrini VoruBelum ada peringkat
- Get in Shape Month2Dokumen5 halamanGet in Shape Month2Caroline Sandry100% (1)
- 8 Surgical Anatomy of TMJDokumen11 halaman8 Surgical Anatomy of TMJArchanaShenoyBelum ada peringkat
- 1.1 Liver Function Tests 15.02.19Dokumen39 halaman1.1 Liver Function Tests 15.02.19Syed ArefinBelum ada peringkat
- Aortic AneurysmDokumen26 halamanAortic Aneurysmchetanm2563100% (1)
- Paediatric Clerking SheetDokumen5 halamanPaediatric Clerking SheetIamTinesh100% (2)
- Gastric Function TestsDokumen5 halamanGastric Function TestssajjadBelum ada peringkat
- 1 BloodDokumen77 halaman1 BloodVisaNathan100% (1)
- @MedicalBooksStore 2015 Office Based PDFDokumen237 halaman@MedicalBooksStore 2015 Office Based PDFGalih WicaksonoBelum ada peringkat
- Child's HerniaDokumen13 halamanChild's HerniaKreshnik HAJDARIBelum ada peringkat
- Applications of EnzymesDokumen33 halamanApplications of EnzymesRoyal Mind100% (1)
- Physiology of Digestion 2014Dokumen58 halamanPhysiology of Digestion 2014sherumar0% (1)
- Hema Ii Laboratory Week 7 - PT & PTT MethodsDokumen37 halamanHema Ii Laboratory Week 7 - PT & PTT MethodsAl-hadad AndromacheBelum ada peringkat
- Nursing Information SystemDokumen20 halamanNursing Information SystemShahad Hakimuddin100% (1)
- PMDC 3rd - Schedule NotifiedDokumen132 halamanPMDC 3rd - Schedule NotifiedMariaLakhaniBelum ada peringkat
- Presented By, N. Swetha M.SC Medical BiochemistryDokumen47 halamanPresented By, N. Swetha M.SC Medical BiochemistryKuzhandai Velu100% (1)
- GERD ManagementDokumen43 halamanGERD ManagementpashaBelum ada peringkat
- Prof. Mutti Ullah Khan Medical Unit III Services HospitalDokumen41 halamanProf. Mutti Ullah Khan Medical Unit III Services HospitalMusa AzharBelum ada peringkat
- Gastric Function Test.... RohitDokumen28 halamanGastric Function Test.... RohitJr Jc Rohit SahBelum ada peringkat
- Healthy Life Style - ModificationDokumen54 halamanHealthy Life Style - ModificationGeorge George100% (1)
- Mechanism of Gastric SecretionDokumen11 halamanMechanism of Gastric Secretionmulya ningsihBelum ada peringkat
- Gastric Function TestsDokumen3 halamanGastric Function TestssreekanthpgBelum ada peringkat
- Chapter 2 BIOCHEMDokumen50 halamanChapter 2 BIOCHEMDentist_2011Belum ada peringkat
- Popular 2Dokumen30 halamanPopular 2Mujahid MehdiBelum ada peringkat
- Bench Marking PresentationDokumen10 halamanBench Marking PresentationbudimanstefanusBelum ada peringkat
- Cyanmethemoglobin Refers To A Relatively NonDokumen5 halamanCyanmethemoglobin Refers To A Relatively NonZahir Jayvee Gayak IIBelum ada peringkat
- AkiDokumen13 halamanAkiharshe v100% (1)
- What Should Not You Do in A Research?Dokumen27 halamanWhat Should Not You Do in A Research?Mohd HardyBelum ada peringkat
- Allergy: Pharm .D, M. Phil Lecturer (Pharmacognosy)Dokumen35 halamanAllergy: Pharm .D, M. Phil Lecturer (Pharmacognosy)Ahmed Imran0% (1)
- Introduction To HAP: by Dr. Mrs. Deepa K. Ingawale (Mandlik) Department of Pharmacology Poona College of Pharmacy, PuneDokumen47 halamanIntroduction To HAP: by Dr. Mrs. Deepa K. Ingawale (Mandlik) Department of Pharmacology Poona College of Pharmacy, PunePrathi100% (2)
- Taenia SpeciesDokumen25 halamanTaenia SpeciesMark Arlo Hernandez SegundoBelum ada peringkat
- Estimation of PCV by Wintrobe MethodDokumen18 halamanEstimation of PCV by Wintrobe Methodjyoti singhBelum ada peringkat
- 5.hafta Ingilizce Bik Pratik-3Dokumen7 halaman5.hafta Ingilizce Bik Pratik-3ManjuBelum ada peringkat
- Platelet Function Tests - DR Makboul 2018 PDFDokumen50 halamanPlatelet Function Tests - DR Makboul 2018 PDFmagendi indra muktiBelum ada peringkat
- Elisa & RiaDokumen4 halamanElisa & Riadihajum3Belum ada peringkat
- WEEK 9 Sterilization & DisinfectionDokumen38 halamanWEEK 9 Sterilization & DisinfectionotaibynaifBelum ada peringkat
- Benchmarking: by Aida TUFEK, 56410921Dokumen58 halamanBenchmarking: by Aida TUFEK, 56410921Aida TufekBelum ada peringkat
- Term Paper ON: Correlation Between Rapid Test and Automated Methods in Diagnosing Infectious Disease Like TyphoidDokumen22 halamanTerm Paper ON: Correlation Between Rapid Test and Automated Methods in Diagnosing Infectious Disease Like TyphoidSoniya DhyaniBelum ada peringkat
- Vitamins ReviewDokumen105 halamanVitamins Reviewjltrek123Belum ada peringkat
- ABO Blood Group System. LegitDokumen11 halamanABO Blood Group System. LegitShestrelmay Launico UmingaBelum ada peringkat
- Mechanism of Hormone ActionDokumen2 halamanMechanism of Hormone Actionegfr3yfgBelum ada peringkat
- Urinalysis: Ms - Deeptikukreti M.SC (N) 1 Year Student RconDokumen20 halamanUrinalysis: Ms - Deeptikukreti M.SC (N) 1 Year Student RconDeepti KukretiBelum ada peringkat
- Basic Immunology Introduction:: Hypersensitivity ReactionsDokumen10 halamanBasic Immunology Introduction:: Hypersensitivity ReactionsRashed ShatnawiBelum ada peringkat
- WBC MorphologyDokumen10 halamanWBC MorphologyGlucose DRglucoseBelum ada peringkat
- HematuriaDokumen51 halamanHematuriaRam ManoharBelum ada peringkat
- Chemical Method of Sterilization - Pharmaceutics IVDokumen6 halamanChemical Method of Sterilization - Pharmaceutics IV03365985198Belum ada peringkat
- Water and Electrolyte Balance Case StudyDokumen3 halamanWater and Electrolyte Balance Case Studyzamadula100% (3)
- Antiadrenergic Drugs 23.07.018 PDFDokumen23 halamanAntiadrenergic Drugs 23.07.018 PDFHitesh karnBelum ada peringkat
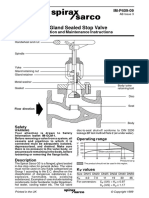
- G3 Gland Sealed Stop Valve-Installation Maintenance Manual PDFDokumen2 halamanG3 Gland Sealed Stop Valve-Installation Maintenance Manual PDFchanBelum ada peringkat
- Pressurized Solar Water HeaterDokumen6 halamanPressurized Solar Water HeaterAlizaIbrahimBelum ada peringkat
- GalactosemiaDokumen3 halamanGalactosemianyx001Belum ada peringkat
- Faecal AnalysisDokumen83 halamanFaecal AnalysisJoseph SabidoBelum ada peringkat
- The Periodic Acid-Schiff (PAS) TechniqueDokumen18 halamanThe Periodic Acid-Schiff (PAS) TechniquevikasBelum ada peringkat
- Pap Smear: Dr. Monika NemaDokumen114 halamanPap Smear: Dr. Monika NemafadoBelum ada peringkat
- All About Pakistan Information McqsDokumen7 halamanAll About Pakistan Information McqsMz ShahBelum ada peringkat
- Cough: PHR Sangita ShakyaDokumen21 halamanCough: PHR Sangita ShakyaCurex QABelum ada peringkat
- Types of FermentersDokumen3 halamanTypes of FermentersHoney krishnaBelum ada peringkat
- Significant Changes From The 2009 Icc To 2012Dokumen87 halamanSignificant Changes From The 2009 Icc To 2012Vịt BầuBelum ada peringkat
- Bench MarkingDokumen10 halamanBench MarkingKrishnaveni MurugeshBelum ada peringkat
- Evaluation of Liver FunctionDokumen64 halamanEvaluation of Liver FunctionMustafa KhandgawiBelum ada peringkat
- Examination of UrineDokumen18 halamanExamination of UrineDr. Jayesh PatidarBelum ada peringkat
- Biological Hazard: Presented by Group 7 Cayamdas, Aimee Castillo, Marie Galleon, Cearlene Santos, KevinDokumen31 halamanBiological Hazard: Presented by Group 7 Cayamdas, Aimee Castillo, Marie Galleon, Cearlene Santos, KevinCearlene GalleonBelum ada peringkat
- Presented By: Khadeeja IkramDokumen49 halamanPresented By: Khadeeja IkramMuhammad JamalBelum ada peringkat
- Anatomy of The KidneysDokumen7 halamanAnatomy of The KidneysSanthu SuBelum ada peringkat
- Water Soluble VitaminsDokumen60 halamanWater Soluble Vitaminsapi-19859346Belum ada peringkat
- Blood GasDokumen9 halamanBlood GasNabila Souza NugrahaBelum ada peringkat
- Drowning: DR K.B.Suryakumar Prof & HOD Dept of Forensic Medicine KVG Medical College Sullia - KarnatakaDokumen33 halamanDrowning: DR K.B.Suryakumar Prof & HOD Dept of Forensic Medicine KVG Medical College Sullia - KarnatakaSuryakumar KilarBelum ada peringkat
- Lec 2 - GIT DrugsDokumen68 halamanLec 2 - GIT DrugsAiqa QaziBelum ada peringkat
- Modell SkellefteaDokumen96 halamanModell SkellefteaMan ManBelum ada peringkat
- MRCPass Notes For MRCP 1 - HEMATOLOGYDokumen9 halamanMRCPass Notes For MRCP 1 - HEMATOLOGYsabdali100% (1)
- 2.PCC Bp3iDokumen36 halaman2.PCC Bp3iRSUD INDRAMAYU PMKPBelum ada peringkat
- Understanding Basics of EKG: by Alula A. (R III)Dokumen37 halamanUnderstanding Basics of EKG: by Alula A. (R III)sky nutsBelum ada peringkat
- PD 03-2020 PDFDokumen2 halamanPD 03-2020 PDFtimvrghs123Belum ada peringkat
- History of Powerlifting Warpeha 9-4-15Dokumen19 halamanHistory of Powerlifting Warpeha 9-4-15Treinador Bruno FerreiraBelum ada peringkat
- Music Therapy Improves Sleep Quality in Acute and ChronicDokumen12 halamanMusic Therapy Improves Sleep Quality in Acute and ChronicLaras Ciingu SyahrezaBelum ada peringkat
- T 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue FeverDokumen2 halamanT 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue Feversamantha cortezBelum ada peringkat
- Mary Oliver - US History Final ProjectDokumen6 halamanMary Oliver - US History Final ProjectMary OliverBelum ada peringkat
- Fucidin® OintDokumen1 halamanFucidin® OintIanthe SinghBelum ada peringkat
- AscarisDokumen16 halamanAscarisRommy Kurniawan DeskyBelum ada peringkat
- Orotol Plus GB 0118Dokumen16 halamanOrotol Plus GB 0118rahmatBelum ada peringkat
- Ineffective Health MaintenanceDokumen6 halamanIneffective Health MaintenanceRYAN SAPLADBelum ada peringkat
- The Tactical Combat Casualty Care Casualty Card - TCCC Guidelines - Proposed Change 1301Dokumen9 halamanThe Tactical Combat Casualty Care Casualty Card - TCCC Guidelines - Proposed Change 1301Paschalis DevranisBelum ada peringkat
- Functions of Liver and GallbladderDokumen10 halamanFunctions of Liver and GallbladderSabiha WaseemBelum ada peringkat
- Compatibility Between Space Analysis Methods of Kesling and Arch Length DiscrepancyDokumen6 halamanCompatibility Between Space Analysis Methods of Kesling and Arch Length DiscrepancynostaBelum ada peringkat
- L10 ToleranceDokumen19 halamanL10 Tolerancesara garciaBelum ada peringkat
- Good Opinion Essay TopicsDokumen4 halamanGood Opinion Essay Topicsmywofod1nud2100% (2)
- Reverse TsaDokumen4 halamanReverse Tsaprwill00Belum ada peringkat