Anda mungkin juga menyukai
- Eating To Win: Activity, Diet and Weight ControlDokumen23 halamanEating To Win: Activity, Diet and Weight ControlAbraham SolomonBelum ada peringkat
- RCT Dimenhydrinate in Children With Infectious Gastroenteritis: A ProspectiveDokumen13 halamanRCT Dimenhydrinate in Children With Infectious Gastroenteritis: A ProspectiveNamira AhmedBelum ada peringkat
- Guarino 2014Dokumen21 halamanGuarino 2014ChangBelum ada peringkat
- Probiotics and Child Care Absence Due To Infections: A Randomized Controlled TrialDokumen11 halamanProbiotics and Child Care Absence Due To Infections: A Randomized Controlled TrialMuhammad FebrianBelum ada peringkat
- Probiotics in Late Infancy Reduce The Incidence of Eczema: A Randomized Controlled TrialDokumen6 halamanProbiotics in Late Infancy Reduce The Incidence of Eczema: A Randomized Controlled TrialarditaBelum ada peringkat
- Oral Ondansetron For Paediatric Gastroenteritis in Primary Care A Randomised Controlled TrialDokumen8 halamanOral Ondansetron For Paediatric Gastroenteritis in Primary Care A Randomised Controlled TrialAssyifa LunaBelum ada peringkat
- Xylitol Syrup For The Prevention of Acute Otitis Media: PediatricsDokumen9 halamanXylitol Syrup For The Prevention of Acute Otitis Media: PediatricsholaBelum ada peringkat
- The Effect of Thickened-Feed Interventions On Gastroesophageal RefluxDokumen13 halamanThe Effect of Thickened-Feed Interventions On Gastroesophageal Refluxminerva_stanciuBelum ada peringkat
- Harding Brits Sunflower 2009Dokumen4 halamanHarding Brits Sunflower 2009Natalia MutahangBelum ada peringkat
- PYMS TamizajeDokumen6 halamanPYMS TamizajeKevinGallagherBelum ada peringkat
- Homeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisDokumen10 halamanHomeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisCarlos Arturo Vera VásquezBelum ada peringkat
- Fermented Milk ComsuptionDokumen10 halamanFermented Milk Comsuptionsilvio da costa guerreiroBelum ada peringkat
- A Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisDokumen11 halamanA Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisErwin YanthoBelum ada peringkat
- Peds 2012-1835Dokumen8 halamanPeds 2012-1835Naraianne FerreiraBelum ada peringkat
- Ems 113478Dokumen16 halamanEms 113478AfniBelum ada peringkat
- ICCH12 JohansenDokumen2 halamanICCH12 Johansenevi_atunBelum ada peringkat
- Screening Neonatal PDFDokumen12 halamanScreening Neonatal PDFDarly ReveloBelum ada peringkat
- TugasDokumen12 halamanTugasLola SantiaBelum ada peringkat
- Bowel Preparations For Colonoscopy: An RCT: AuthorsDokumen10 halamanBowel Preparations For Colonoscopy: An RCT: AuthorsCalvin AffendyBelum ada peringkat
- 10 1111@pedi 12777Dokumen10 halaman10 1111@pedi 12777MahmudahBelum ada peringkat
- Diarrhea in Preschool Children and Lactobacillus 2017Dokumen9 halamanDiarrhea in Preschool Children and Lactobacillus 2017Karindha Handayani HelisusantoBelum ada peringkat
- General Practice: Are Antibiotics Indicated As Initial Treatment For Children With Acute Otitis Media? A Meta-AnalysisDokumen5 halamanGeneral Practice: Are Antibiotics Indicated As Initial Treatment For Children With Acute Otitis Media? A Meta-AnalysisJuan Carlos Aguayo RomeroBelum ada peringkat
- Pediatric Gastroesophageal Reflux DiseaseDokumen5 halamanPediatric Gastroesophageal Reflux Diseasegemala wahabBelum ada peringkat
- Pneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredDokumen9 halamanPneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredSulis Na EndutzBelum ada peringkat
- Oral Administration of Tannins and Flavonoids in Children With Acute Diarrhea: A Pilot, Randomized, Control-Case StudyDokumen6 halamanOral Administration of Tannins and Flavonoids in Children With Acute Diarrhea: A Pilot, Randomized, Control-Case StudyAnonymous jM0QFnr0Belum ada peringkat
- Direct Hyperbilirubinemia in Newborns With GastroschisisDokumen9 halamanDirect Hyperbilirubinemia in Newborns With GastroschisisAnisaa GayatriBelum ada peringkat
- Clinical Reviews: The Management of Children With Gastroenteritis and Dehydration in The Emergency DepartmentDokumen13 halamanClinical Reviews: The Management of Children With Gastroenteritis and Dehydration in The Emergency DepartmentRina Dewi AnggraeniBelum ada peringkat
- EDA. Pediatrics 2010Dokumen12 halamanEDA. Pediatrics 2010Carkos MorenoBelum ada peringkat
- Lactobacillus Therapy For Acute Infectious Diarrhea in Children A Meta-AnalysisDokumen9 halamanLactobacillus Therapy For Acute Infectious Diarrhea in Children A Meta-AnalysisfahrunisaBelum ada peringkat
- Articulos BronquiolitisDokumen18 halamanArticulos BronquiolitisLaura López Del Castillo LalydelcaBelum ada peringkat
- Clinical Nutrition: Randomized Control TrialsDokumen5 halamanClinical Nutrition: Randomized Control TrialsBby AdelinaBelum ada peringkat
- Jurnal PediatriDokumen11 halamanJurnal PediatriKoas PatoBelum ada peringkat
- Lactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenDokumen21 halamanLactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenMarsella Epifania SuwignyoBelum ada peringkat
- By Guest On July 22, 2019 Downloaded FromDokumen3 halamanBy Guest On July 22, 2019 Downloaded FromNoviaBelum ada peringkat
- Can A Flavored Spray (Pill Glide) Help Children Swallow Their Medicines? A Pilot StudyDokumen11 halamanCan A Flavored Spray (Pill Glide) Help Children Swallow Their Medicines? A Pilot StudyUmar AliBelum ada peringkat
- JN 212308Dokumen8 halamanJN 212308Ivhajannatannisa KhalifatulkhusnulkhatimahBelum ada peringkat
- 19d. CPG Article - ESPGHAN 2008Dokumen42 halaman19d. CPG Article - ESPGHAN 2008Aditya Angela AdamBelum ada peringkat
- Hyperbilirubinemia, Phototherapy, and Childhood Asthma: ObjectivesDokumen11 halamanHyperbilirubinemia, Phototherapy, and Childhood Asthma: ObjectivesrizaniaBelum ada peringkat
- Homeopathic Treatment of Acute Childhood Diarrhea: Results From A Clinical Trial in NepalDokumen10 halamanHomeopathic Treatment of Acute Childhood Diarrhea: Results From A Clinical Trial in NepalKiran DalabanjanBelum ada peringkat
- What Is The Role of Antiemetics For Children With Acute Gastroenteritis in The Developing World?Dokumen4 halamanWhat Is The Role of Antiemetics For Children With Acute Gastroenteritis in The Developing World?Shafa AudryBelum ada peringkat
- Pediatrics 2014 Queen E23 9Dokumen10 halamanPediatrics 2014 Queen E23 9Desrainy InhardiniBelum ada peringkat
- Early Analgesia For Children With Acute Abdominal Pain: ObjectivesDokumen8 halamanEarly Analgesia For Children With Acute Abdominal Pain: Objectivescrizt tyanBelum ada peringkat
- Acute Gastroenteritis in Children of The World: What Needs To Be Done?Dokumen8 halamanAcute Gastroenteritis in Children of The World: What Needs To Be Done?yoonie catBelum ada peringkat
- Jurnal PJJ WordDokumen21 halamanJurnal PJJ WordnanamirBelum ada peringkat
- Does This Child Have Appendicitis?: The Rational Clinical ExaminationDokumen14 halamanDoes This Child Have Appendicitis?: The Rational Clinical ExaminationTrys RobledoBelum ada peringkat
- 2012 ESPGHAN Recommendations On Infection and Prevention JPGN PDFDokumen8 halaman2012 ESPGHAN Recommendations On Infection and Prevention JPGN PDFAna Clara ReisBelum ada peringkat
- Thyroid ReviewDokumen45 halamanThyroid ReviewSharin K VargheseBelum ada peringkat
- Infantile Hypertrophic Pyloric Stenosis at A TertiDokumen7 halamanInfantile Hypertrophic Pyloric Stenosis at A TertiVașadi Razvan CristianBelum ada peringkat
- Diarrhea, Dehydration, and The Associated Mortality in Children With Complicated Severe Acute Malnutrition: A Prospective Cohort Study in UgandaDokumen11 halamanDiarrhea, Dehydration, and The Associated Mortality in Children With Complicated Severe Acute Malnutrition: A Prospective Cohort Study in Ugandasalma romnalia ashshofaBelum ada peringkat
- Childhood Urinary Tract Infection in Primary Care:: ResearchDokumen7 halamanChildhood Urinary Tract Infection in Primary Care:: ResearchLavfy NjlaaBelum ada peringkat
- Intestinal Probiotics in Relieving Clinical Symptoms of Severe Hand, Foot and Mouth Desease and Potential Mechanism AnalysisDokumen6 halamanIntestinal Probiotics in Relieving Clinical Symptoms of Severe Hand, Foot and Mouth Desease and Potential Mechanism AnalysisJUAN SEBASTIAN AVELLANEDA MARTINEZBelum ada peringkat
- Efficacy of Propranolol Between 6 and 12 Months of Age in High Risk Infantile HemangiomDokumen10 halamanEfficacy of Propranolol Between 6 and 12 Months of Age in High Risk Infantile HemangiomNoviaBelum ada peringkat
- Current Success in The Treatment of Intussusception in ChildrenDokumen9 halamanCurrent Success in The Treatment of Intussusception in ChildrenOby RomdhoniBelum ada peringkat
- Colletti2010 PDFDokumen13 halamanColletti2010 PDFBrayan Hidalgo AmasifuenBelum ada peringkat
- Epinephrine and Dexamethasone in Children With BronchiolitisDokumen11 halamanEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisBelum ada peringkat
- Gastroentritis AcuteDokumen10 halamanGastroentritis AcuteYN Eyin VelinBelum ada peringkat
- Zinc As An Adjunct Therapy in The Management of Severe Pneumonia Among Gambian Children: Randomized Controlled TrialDokumen19 halamanZinc As An Adjunct Therapy in The Management of Severe Pneumonia Among Gambian Children: Randomized Controlled TrialDicky rahadianBelum ada peringkat
- PapersDokumen5 halamanPapersAldora OktavianaBelum ada peringkat
- Infant Gastroesophageal Reflux Disease Management Consensus 2024Dokumen8 halamanInfant Gastroesophageal Reflux Disease Management Consensus 2024Dayana FajardoBelum ada peringkat
- Endoscopy in Pediatric Inflammatory Bowel DiseaseDari EverandEndoscopy in Pediatric Inflammatory Bowel DiseaseLuigi Dall'OglioBelum ada peringkat
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementDari EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornBelum ada peringkat
- 110-Dehydration and Disorders of Sodium BalanceDokumen5 halaman110-Dehydration and Disorders of Sodium BalancepelinBelum ada peringkat
- Oral Rehydration Therapy - UpToDateDokumen16 halamanOral Rehydration Therapy - UpToDateNedelcu MirunaBelum ada peringkat
- Antidiarrhoeal AgentsDokumen14 halamanAntidiarrhoeal AgentsTarek G MustafaBelum ada peringkat
- Nutrient Timing and Training: The Warfighter Nutrition GuideDokumen15 halamanNutrient Timing and Training: The Warfighter Nutrition GuideBenBelum ada peringkat
- Oral Rehydration TherapyDokumen42 halamanOral Rehydration TherapyGaurav GuptaBelum ada peringkat
- Dietary Management in Disease - IDokumen28 halamanDietary Management in Disease - IPriya SoniBelum ada peringkat
- Articulo Sobre La Sobada en Costa RicaDokumen5 halamanArticulo Sobre La Sobada en Costa RicaJavierCalderónGutiérrezBelum ada peringkat
- Diarrhoea in PediatricsDokumen89 halamanDiarrhoea in PediatricsKimbek BuangkeBelum ada peringkat
- Acute Gastroenteritis in Children: Prepared By: Prof. Elizabeth D. Cruz RN, ManDokumen12 halamanAcute Gastroenteritis in Children: Prepared By: Prof. Elizabeth D. Cruz RN, ManChaii De GuzmanBelum ada peringkat
- Management of Acute Gastroenteritis in ChildrenDokumen14 halamanManagement of Acute Gastroenteritis in ChildrenYayaBelum ada peringkat
- Fluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationDokumen195 halamanFluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationNayely MoralesBelum ada peringkat
- Add (Acute Diarrhoeal Disease)Dokumen46 halamanAdd (Acute Diarrhoeal Disease)Mohamed Mahroof100% (1)
- Ethiopia Guidelines For AM August 19082019Dokumen157 halamanEthiopia Guidelines For AM August 19082019Lavinia BaleaBelum ada peringkat
- Dehydration Isonatremic, Hyponatremic, andDokumen15 halamanDehydration Isonatremic, Hyponatremic, andalfredoibcBelum ada peringkat
- Nutritional Applications in Exercise and Sport PDFDokumen309 halamanNutritional Applications in Exercise and Sport PDFalexceseBelum ada peringkat
- ORS Package InsertDokumen1 halamanORS Package InsertwhothehellisarcticmonkeysBelum ada peringkat
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDokumen20 halamanLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuBelum ada peringkat
- A Clinical Report On Field Attachment at Matungu Sub - County HospitalDokumen46 halamanA Clinical Report On Field Attachment at Matungu Sub - County HospitalJustin 037Belum ada peringkat
- Cholera Kits 2021 Content 20.02.2024 Rev LabDokumen37 halamanCholera Kits 2021 Content 20.02.2024 Rev LabElom Kokou ASSIGBLEY100% (1)
- Management of The Short Bowel Syndrome in Adults - UpToDateDokumen10 halamanManagement of The Short Bowel Syndrome in Adults - UpToDateyessyBelum ada peringkat
- IntussusceptionDokumen2 halamanIntussusceptionrising starBelum ada peringkat
- Frequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaDokumen4 halamanFrequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaRaja Bajak LautBelum ada peringkat
- PharmCal Lab Finals (H2O2, Alum, Aluminum Magnesium Hydoxide Gel, ORS, Cupric Sulfate)Dokumen10 halamanPharmCal Lab Finals (H2O2, Alum, Aluminum Magnesium Hydoxide Gel, ORS, Cupric Sulfate)a yellow flowerBelum ada peringkat
- How To Replace Lost ElectrolytesDokumen3 halamanHow To Replace Lost ElectrolytesSridhar ChBelum ada peringkat
- Fluid Treatment Pattern VSDokumen8 halamanFluid Treatment Pattern VSDen PeraBelum ada peringkat
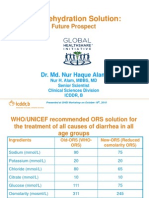
- Oral Rehydration Solution:: Future ProspectDokumen48 halamanOral Rehydration Solution:: Future ProspectmustikaarumBelum ada peringkat
- Presentation DiarrheaDokumen23 halamanPresentation DiarrheaVenkatesh KS 233Belum ada peringkat
- On-Going AppraisalDokumen9 halamanOn-Going AppraisaltrishaBelum ada peringkat
- Diare Dan DehidrasiDokumen61 halamanDiare Dan DehidrasiOktavian Rizki IlahiBelum ada peringkat