Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- 16S Metagenomic Analysis TutorialDokumen9 halaman16S Metagenomic Analysis TutorialJack SimBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- ALS Reversals Demographics Disease Characteristics Treatments and Co MorbiditiesDokumen6 halamanALS Reversals Demographics Disease Characteristics Treatments and Co MorbiditiesJoseaneBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Options To Improve The Action of PROTACs in Cancer Development of Controlled Delivery NanoparticlesDokumen13 halamanOptions To Improve The Action of PROTACs in Cancer Development of Controlled Delivery NanoparticlesHan GaoBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- AIChE Pocket HandbookDokumen64 halamanAIChE Pocket HandbookDinesh KanaujiyaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Nanotechnology: Done By-Naveeshi Lawanya, Samadhee Kiriwandalage and Minduli MedagodaDokumen13 halamanNanotechnology: Done By-Naveeshi Lawanya, Samadhee Kiriwandalage and Minduli Medagodanalinda medagodaBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Humanistic Learning Theori - 1 PDFDokumen24 halamanHumanistic Learning Theori - 1 PDFEka Wahyu NurlailiBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Science Form 3 Chapter 3: Name: Class: DateDokumen6 halamanScience Form 3 Chapter 3: Name: Class: DateTeng Pei ErBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Pro-Bio Beads: Solgar Vitamin and HerbDokumen2 halamanPro-Bio Beads: Solgar Vitamin and HerbM Usman KhanBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Curvas de RarefacciónDokumen3 halamanCurvas de RarefacciónRoberto Flores CruzBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- 2005 Report PDFDokumen181 halaman2005 Report PDFlokmatgroup3660Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
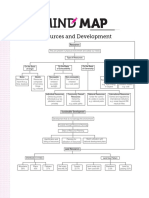
- MindmapDokumen1 halamanMindmapSwapnil Tak25% (4)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- College of Medical Laboratory Science Our Lady of Fatima University-VelenzuelaDokumen33 halamanCollege of Medical Laboratory Science Our Lady of Fatima University-VelenzuelaClaire GonoBelum ada peringkat
- Breakthrough Microbiome-Based Solutions: TargedysDokumen4 halamanBreakthrough Microbiome-Based Solutions: TargedysSandraJSantosBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Phylogeny and EvolutionDokumen12 halamanPhylogeny and EvolutionKathryn Palmerton0% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- 2021-22 Extract-from-Annual-Report-DanishDokumen24 halaman2021-22 Extract-from-Annual-Report-DanishDavidBelum ada peringkat
- 02 WholeDokumen254 halaman02 WholeSwift Tailor GameBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- A Compilation of Philippine Environmental LawsDokumen39 halamanA Compilation of Philippine Environmental LawsRussel Sirot100% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Edwards - Categories Are For Talking T&P 1991Dokumen26 halamanEdwards - Categories Are For Talking T&P 1991txthedxBelum ada peringkat
- The Physic Body MechanicsDokumen8 halamanThe Physic Body MechanicsNur RasyiqahBelum ada peringkat
- LEARNING MODULE - SCIENCE 9 - MODULE 3 - Q1 - W3 NEW OkDokumen9 halamanLEARNING MODULE - SCIENCE 9 - MODULE 3 - Q1 - W3 NEW OkMatt Mc Henry HernandezBelum ada peringkat
- Curriculum VitaeDokumen3 halamanCurriculum Vitaeanon-866464Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Selander 1991 - On The Nomenclature and Classification of The MeloidaeDokumen31 halamanSelander 1991 - On The Nomenclature and Classification of The MeloidaecristianBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Structure and Function of Prokaryotic Cells: Lecture Number 2: TopicsDokumen2 halamanStructure and Function of Prokaryotic Cells: Lecture Number 2: Topicsalex zhangBelum ada peringkat
- Guia MyaDokumen6 halamanGuia MyaPedro A. MartinezBelum ada peringkat
- Child Development GROUP SOPHIEDokumen30 halamanChild Development GROUP SOPHIESyazwani ZainalBelum ada peringkat
- Barrett's EsophagusDokumen10 halamanBarrett's EsophagusaryadroettninguBelum ada peringkat
- Module 3Dokumen15 halamanModule 3RabbitFamBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Muscular TissueDokumen6 halamanMuscular TissueChezkaMayC.OliverosBelum ada peringkat
- 2016 - Chuyên Thái NguyênDokumen12 halaman2016 - Chuyên Thái NguyênRoland VietnamBelum ada peringkat
- As Cell MembranesDokumen27 halamanAs Cell MembranesNoel Johansen-BergBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)