Anda mungkin juga menyukai
- The Chairs by Eugene IonescoDokumen6 halamanThe Chairs by Eugene IonescoAndrea Rosialda100% (1)
- Vahan 4Dokumen1 halamanVahan 4BhushanBelum ada peringkat
- 80D Pdf-AnkitDokumen1 halaman80D Pdf-AnkitSaurabh RaghuvanshiBelum ada peringkat
- SBI LIFE Premium CertificateDokumen1 halamanSBI LIFE Premium CertificatearithotiBelum ada peringkat
- ICICI Premium - HemavathyDokumen2 halamanICICI Premium - HemavathyAshok SBelum ada peringkat
- In - Gov.transport RVCER TN01BK9115Dokumen1 halamanIn - Gov.transport RVCER TN01BK9115Dr. Ezaykiyel PTBelum ada peringkat
- Reg No: Dl8Cav0116: Registration Certificate For VehicleDokumen1 halamanReg No: Dl8Cav0116: Registration Certificate For Vehicleh4ckerBelum ada peringkat
- Premium Paid CertificateDokumen1 halamanPremium Paid CertificateSenthil balasubramanianBelum ada peringkat
- Premium Paid AcknowledgementDokumen1 halamanPremium Paid AcknowledgementAtreya ChakrobortyBelum ada peringkat
- Read Aloud Plan (3105) : StandardsDokumen3 halamanRead Aloud Plan (3105) : Standardsapi-490091219Belum ada peringkat
- Sample Test Paper 3 USE OF ENGLISH (30 Minutes)Dokumen5 halamanSample Test Paper 3 USE OF ENGLISH (30 Minutes)Lau RamirezBelum ada peringkat
- Israel's Story in Maps Pt2Dokumen15 halamanIsrael's Story in Maps Pt2Israel-Is100% (5)
- Honda Elite Manual DespieceDokumen4 halamanHonda Elite Manual DespieceLeonidas Zapata OlivaresBelum ada peringkat
- Disability Certificate FormatDokumen2 halamanDisability Certificate FormatTheertha Prasad100% (2)
- Pawan S PDF CompletedDokumen1 halamanPawan S PDF CompletedAsifshaikh7566Belum ada peringkat
- PrmPayRcptSign PR0445228800021011Dokumen1 halamanPrmPayRcptSign PR0445228800021011dipakpd100% (1)
- RAJU CertificateDokumen1 halamanRAJU CertificateSuhail KhanBelum ada peringkat
- MedicalimDokumen1 halamanMedicalimsaurabhBelum ada peringkat
- Person With Disability RegistrationDokumen2 halamanPerson With Disability RegistrationSelvakumar KumarBelum ada peringkat
- Ashwani KumarDokumen1 halamanAshwani KumarTarunBelum ada peringkat
- Renewal NoticeDokumen2 halamanRenewal NoticeJerry LamaBelum ada peringkat
- 1865362Dokumen1 halaman1865362Bhavesh ParekhBelum ada peringkat
- Premium Paid CertificateDokumen1 halamanPremium Paid CertificateVishal DBelum ada peringkat
- For HDFC ERGO General Insurance Company LTDDokumen2 halamanFor HDFC ERGO General Insurance Company LTDNAVEEN H EBelum ada peringkat
- Certificate For Person With Disability: Government of Andhra PradeshDokumen1 halamanCertificate For Person With Disability: Government of Andhra Pradeshనీలం మధు సూధన్ రెడ్డిBelum ada peringkat
- 80D SelfDokumen1 halaman80D Selfnikhil nadakuditiBelum ada peringkat
- Premium Paid Certificate: Date: 14-DEC-2017Dokumen1 halamanPremium Paid Certificate: Date: 14-DEC-2017zuhebBelum ada peringkat
- Shri Mata Vaishno Devi Shrine BoardDokumen1 halamanShri Mata Vaishno Devi Shrine BoardDivine NatureBelum ada peringkat
- FeeReceipt Sep2019Dokumen1 halamanFeeReceipt Sep2019KavitaBelum ada peringkat
- LIC Sikha PDFDokumen1 halamanLIC Sikha PDFsikha singh100% (1)
- 80EEA DeclarationDokumen1 halaman80EEA DeclarationNAGARJUNABelum ada peringkat
- Subject: Risk Assumption Letter: LAN Number: 19020618531140 Policy Number: 4111/EPP/164559158/00/000Dokumen2 halamanSubject: Risk Assumption Letter: LAN Number: 19020618531140 Policy Number: 4111/EPP/164559158/00/000shekarBelum ada peringkat
- TG1628 School Fees I PDFDokumen1 halamanTG1628 School Fees I PDFAnandKumarPBelum ada peringkat
- Dengue Ns1 Antigen Test (Elisa/Elfa) - 600.00 0.00: DuplicateDokumen1 halamanDengue Ns1 Antigen Test (Elisa/Elfa) - 600.00 0.00: DuplicateAbhishek GoelBelum ada peringkat
- Leave and License Agreement: Particulars Amount Paid GRN/Transaction Id DateDokumen6 halamanLeave and License Agreement: Particulars Amount Paid GRN/Transaction Id DateAnonymous eCmTYonQ84Belum ada peringkat
- Tax Certificate - 008927742 - 131310Dokumen2 halamanTax Certificate - 008927742 - 131310Vignesh MahadevanBelum ada peringkat
- Policy CertificateDokumen5 halamanPolicy CertificateRahulpatel25Belum ada peringkat
- AugDokumen1 halamanAugsrikanth0483287Belum ada peringkat
- Health DocumentDokumen2 halamanHealth Documentramki240Belum ada peringkat
- Consolidated Premium Paid STMT 2012-2013Dokumen1 halamanConsolidated Premium Paid STMT 2012-2013jahmeddBelum ada peringkat
- AC Bajaj Finance - 2Dokumen2 halamanAC Bajaj Finance - 2prsnjt11Belum ada peringkat
- The New India Assurance Co. Ltd. (Government of India Undertaking)Dokumen4 halamanThe New India Assurance Co. Ltd. (Government of India Undertaking)Ameya SudameBelum ada peringkat
- 80D CertificateDokumen2 halaman80D CertificateSiva KadaliBelum ada peringkat
- Registration Certificate of Vehicle: Issuing Authority: Madhubani, BiharDokumen1 halamanRegistration Certificate of Vehicle: Issuing Authority: Madhubani, Bihartabrez alamBelum ada peringkat
- Consolidated Premium Paid STMT 2020-2021 PDFDokumen1 halamanConsolidated Premium Paid STMT 2020-2021 PDFSHITESH KUMARBelum ada peringkat
- Please Note This Is A Digitally Signed Invoice.: Original For RecipientDokumen1 halamanPlease Note This Is A Digitally Signed Invoice.: Original For RecipientRajnish JainBelum ada peringkat
- Prashant (1) CompletedDokumen1 halamanPrashant (1) CompletedAsifshaikh7566Belum ada peringkat
- HDFC Ulip 2021-22Dokumen2 halamanHDFC Ulip 2021-22Sandip Kumar Dube100% (1)
- formFeeRecieptPrintReport Duplicate RC Book PDFDokumen1 halamanformFeeRecieptPrintReport Duplicate RC Book PDFsnaehalBelum ada peringkat
- Received With Thanks ' 2,308.00 Through Payment Gateway Over The Internet FromDokumen1 halamanReceived With Thanks ' 2,308.00 Through Payment Gateway Over The Internet FromKumara RagavendraBelum ada peringkat
- Renewal Premium Notice: Mr. Kishor Kumar Gupta Insured Name: MR - Kishor Kumar GuptaDokumen1 halamanRenewal Premium Notice: Mr. Kishor Kumar Gupta Insured Name: MR - Kishor Kumar GuptaYT ENTERTAINMENTBelum ada peringkat
- Indian Income Tax Return Acknowledgement: Do Not Send This Acknowledgement To CPC, BengaluruDokumen1 halamanIndian Income Tax Return Acknowledgement: Do Not Send This Acknowledgement To CPC, Bengalurupatel dharmeshBelum ada peringkat
- Siti Broadband (Sep-Oct) BillDokumen1 halamanSiti Broadband (Sep-Oct) BillBARUN BIKASH DEBelum ada peringkat
- Gym FeesDokumen1 halamanGym FeesMrityunjay AryanBelum ada peringkat
- SaibabaDokumen1 halamanSaibabasameer5458100% (1)
- Max Health InsuranceDokumen1 halamanMax Health InsuranceanuBelum ada peringkat
- Renewal of Your Ican Essential Advanced Insurance PolicyDokumen3 halamanRenewal of Your Ican Essential Advanced Insurance PolicySuganthi ChandrasekaranBelum ada peringkat
- New - Life Insurance Corporation of India - Sowmya - 2023Dokumen1 halamanNew - Life Insurance Corporation of India - Sowmya - 2023boddu sowmyaBelum ada peringkat
- Form No. 10-I: Certificate of Prescribed Authority For The Purposes of Section 80DDBDokumen1 halamanForm No. 10-I: Certificate of Prescribed Authority For The Purposes of Section 80DDBIam KarthikeyanBelum ada peringkat
- Tax ReceiptDokumen1 halamanTax ReceiptSumit SumanBelum ada peringkat
- NPS Account StatementDokumen2 halamanNPS Account Statementdinesh rajendranBelum ada peringkat
- A) Locomotor or Cerebral PalsyDokumen1 halamanA) Locomotor or Cerebral PalsyAnonymous NJDmHvjBelum ada peringkat
- Format of Medical Certificate For Persons With Disabilities (PWD) Name and Address of The Institute/ HospitalDokumen1 halamanFormat of Medical Certificate For Persons With Disabilities (PWD) Name and Address of The Institute/ HospitalYash ManeBelum ada peringkat
- Form For Physically Disabled CategoryDokumen1 halamanForm For Physically Disabled Categoryakbar_hssnBelum ada peringkat
- App IDokumen1 halamanApp IRohit KumarBelum ada peringkat
- Anthropology Is The Ethnography of PhilosophyDokumen3 halamanAnthropology Is The Ethnography of PhilosophyNian PissolatiBelum ada peringkat
- Tom SwayerDokumen34 halamanTom SwayerJæž ËviBelum ada peringkat
- Syllabus FisiotherapyDokumen5 halamanSyllabus FisiotherapyMikki MoriBelum ada peringkat
- Usaha Kesehatan SekolahDokumen36 halamanUsaha Kesehatan SekolahLamlay SarieBelum ada peringkat
- Otto Bohlmann Auth. Yeats and Nietzsche An Exploration of Major Nietzschean Echoes in The Writings of William Butler Yeats PDFDokumen243 halamanOtto Bohlmann Auth. Yeats and Nietzsche An Exploration of Major Nietzschean Echoes in The Writings of William Butler Yeats PDFDanja Tešić100% (1)
- VFB '/iffm KL/JF/SF) '/iff: Kmfob) LV E08F/0F DDDokumen4 halamanVFB '/iffm KL/JF/SF) '/iff: Kmfob) LV E08F/0F DDRajesh KoiralaBelum ada peringkat
- Vant Hoff FactorDokumen1 halamanVant Hoff FactorPlopBelum ada peringkat
- Generating SQL Trace FilesDokumen24 halamanGenerating SQL Trace FilesramaniqbalBelum ada peringkat
- Daftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Dokumen10 halamanDaftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Poliklinik RSPHBelum ada peringkat
- English NcertDokumen152 halamanEnglish NcertYasir SaeedBelum ada peringkat
- CW Grade 9 Module 1Dokumen11 halamanCW Grade 9 Module 1Carla MaglantayBelum ada peringkat
- Bacula For DevelopersDokumen137 halamanBacula For Developersfrederyk83Belum ada peringkat
- Test Cases and Check List Primer Test Kejsa SajtaDokumen11 halamanTest Cases and Check List Primer Test Kejsa SajtaМария ДмитриеваBelum ada peringkat
- Calendar Thematic Plan For Grade 3 Within The Framework of Updating The Secondary Education Content 2021 - 2022 Academic YearDokumen6 halamanCalendar Thematic Plan For Grade 3 Within The Framework of Updating The Secondary Education Content 2021 - 2022 Academic YearAkonya AnarbekovaBelum ada peringkat
- Node-Lock ProceduresDokumen3 halamanNode-Lock ProceduresgeneraljomoBelum ada peringkat
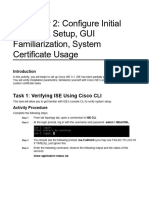
- Discovery 2: Configure Initial Cisco ISE Setup, GUI Familiarization, System Certificate UsageDokumen27 halamanDiscovery 2: Configure Initial Cisco ISE Setup, GUI Familiarization, System Certificate UsagebounprakopBelum ada peringkat
- English Placement TestDokumen49 halamanEnglish Placement TestZin WendyBelum ada peringkat
- Lesson 3Dokumen2 halamanLesson 3RonnieBelum ada peringkat
- SAP1024B v6Dokumen57 halamanSAP1024B v6nhatnam06dt1Belum ada peringkat
- NTH Differentiation ExplainedDokumen9 halamanNTH Differentiation Explainedjoshyw072Belum ada peringkat
- B Tech Courses Ai and DsDokumen168 halamanB Tech Courses Ai and Dsvvaswincode11Belum ada peringkat
- Birth CertificateDokumen3 halamanBirth CertificateDanielBelum ada peringkat
- Joanna Daganta - IER EXAM 2Dokumen4 halamanJoanna Daganta - IER EXAM 2Joanna DagantaBelum ada peringkat
- Tegar Manthofani: Software DeveloperDokumen1 halamanTegar Manthofani: Software DeveloperBagongBelum ada peringkat
- Ielts Online ReferenceDokumen47 halamanIelts Online ReferenceImadeddinBelum ada peringkat