Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Marantz SR 4000 User GuideDokumen30 halamanMarantz SR 4000 User Guidekeerthipinnawala6498100% (1)
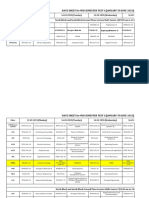
- Date Sheet (MST-I)Dokumen12 halamanDate Sheet (MST-I)Tauqeer AhmadBelum ada peringkat
- Withdrawal Withdrawal Withdrawal WithdrawalDokumen15 halamanWithdrawal Withdrawal Withdrawal WithdrawalAradhya 19-1807Belum ada peringkat
- Bi Weekly Budget TrackerDokumen22 halamanBi Weekly Budget TrackeranamarieBelum ada peringkat
- LP in LogarithmsDokumen5 halamanLP in LogarithmsDon Joey Loyola PontevedraBelum ada peringkat
- JFET AC Equivalent CircuitsDokumen42 halamanJFET AC Equivalent Circuitssakuntala barikBelum ada peringkat
- Basic Discrete StructureDokumen57 halamanBasic Discrete StructureAhmed Iqbal100% (1)
- Forward Error Correction (FEC)Dokumen6 halamanForward Error Correction (FEC)gamer08Belum ada peringkat
- 21 Primavera Tips and ShortcutsDokumen30 halaman21 Primavera Tips and ShortcutsMarioBelum ada peringkat
- Android Voting System Synopsis Under 40 CharactersDokumen3 halamanAndroid Voting System Synopsis Under 40 CharactersShivshankar GuptaBelum ada peringkat
- EADK Architecture GuideDokumen31 halamanEADK Architecture GuideUltrazikingBelum ada peringkat
- SAP SRM 7.0 Strategic SourcingDokumen90 halamanSAP SRM 7.0 Strategic SourcingSergio Martinez PerezBelum ada peringkat
- ENGG103 Course Specifications Eng v202Dokumen7 halamanENGG103 Course Specifications Eng v202Ibrahim MahamidBelum ada peringkat
- Pressure Calibrators: Low, Medium and High PressureDokumen2 halamanPressure Calibrators: Low, Medium and High PressureMarcelo PellizzaBelum ada peringkat
- ISTQB Foundation Exam Format andDokumen17 halamanISTQB Foundation Exam Format andapi-3806986Belum ada peringkat
- Fidelityfx Cas: Lou Kramer, Developer Technology Engineer, AmdDokumen92 halamanFidelityfx Cas: Lou Kramer, Developer Technology Engineer, AmdJohn K SmithBelum ada peringkat
- BN20 e PreDokumen59 halamanBN20 e PreTuan DinhBelum ada peringkat
- Analytics and Maintenance of ICT ProjectsDokumen26 halamanAnalytics and Maintenance of ICT ProjectsK-yanVehraaYomomaBelum ada peringkat
- Lecture - 5: DC-AC Converters: Ug - ProgramDokumen54 halamanLecture - 5: DC-AC Converters: Ug - ProgramArife AbdulkerimBelum ada peringkat
- Ict111 Module 02Dokumen7 halamanIct111 Module 02Cluster 2, Cebu city, Josh C AgustinBelum ada peringkat
- City of Sedona - Wireless Master PlanDokumen136 halamanCity of Sedona - Wireless Master Plana hBelum ada peringkat
- Online Book StoreDokumen36 halamanOnline Book StoreGourab Dey100% (1)
- Pinouts ICRDokumen38 halamanPinouts ICRAdal Vera100% (1)
- III Year SyllabusDokumen68 halamanIII Year SyllabusFaiz KarobariBelum ada peringkat
- UntitledDokumen36 halamanUntitledisaac gonzalezBelum ada peringkat
- ZJ 5780s Instruction BookDokumen102 halamanZJ 5780s Instruction BookRATSITOHARA EricBelum ada peringkat
- Review of Industrial Deployment of Multi-Agent SystemsDokumen24 halamanReview of Industrial Deployment of Multi-Agent SystemsVasant RaghavBelum ada peringkat
- Scripting Language - WikipediaDokumen9 halamanScripting Language - WikipediaGilbertBelum ada peringkat
- PC Programming Manual: KX-TDA30/KX-TDA100 KX-TDA200/KX-TDA600Dokumen842 halamanPC Programming Manual: KX-TDA30/KX-TDA100 KX-TDA200/KX-TDA600anon_588155774Belum ada peringkat
- Ssp393 - Audi A5 - Convenience Electronics and Driver Assist SystemsDokumen56 halamanSsp393 - Audi A5 - Convenience Electronics and Driver Assist SystemsCyberemuleBelum ada peringkat