Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
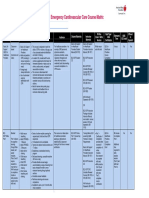
- Emergency Cardiovascular Care Course MatrixDokumen15 halamanEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Levels of EvidenceDokumen4 halamanLevels of EvidenceshineeicaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- EcotherapyDokumen2 halamanEcotherapygeraldinmccaul85Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Psychological AdjustmentDokumen100 halamanPsychological AdjustmentRagil Adist Surya PutraBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Deep Back Massage 3Dokumen11 halamanDeep Back Massage 3Anonymous ecK9pw1O3QBelum ada peringkat
- BPD Concept MapDokumen3 halamanBPD Concept Mapsammillepointer86Belum ada peringkat
- Study: Observational Travelers' DiarrheaDokumen5 halamanStudy: Observational Travelers' DiarrheaFathah MuhammadBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Dialysis Centre: Assignment - 3Dokumen12 halamanDialysis Centre: Assignment - 3grvoneandonlyBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Discharge Planning ProjectDokumen6 halamanDischarge Planning Projectapi-280998981Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- AGMCDokumen38 halamanAGMCsmrutiptBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- ITAT Holds That Charitable Trust Running Max Hospital Was Charitable To Only To Corporate Max Group of Companies and Uncharitable' Towards The Society or PublicDokumen46 halamanITAT Holds That Charitable Trust Running Max Hospital Was Charitable To Only To Corporate Max Group of Companies and Uncharitable' Towards The Society or PublicLive LawBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Faces Iv and The Circumplex Model - Validation Study PDFDokumen17 halamanFaces Iv and The Circumplex Model - Validation Study PDFjulinau25Belum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Management of Failed Block - Harsh.Dokumen48 halamanManagement of Failed Block - Harsh.Faeiz KhanBelum ada peringkat
- Blood Sugar Insulin Polyuria Polydipsia PolyphagiaDokumen7 halamanBlood Sugar Insulin Polyuria Polydipsia PolyphagiankirrBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Adverse Drug Interaction in Dental PracticeDokumen8 halamanAdverse Drug Interaction in Dental PracticeSusanna TsoBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Project Hospital Fin All Business SummaryDokumen32 halamanProject Hospital Fin All Business Summarykanchoo100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Myopia APDF PDFDokumen14 halamanMyopia APDF PDFRao Sab100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Filler Rhinoplasty: Evidence, Outcomes, and ComplicationsDokumen3 halamanFiller Rhinoplasty: Evidence, Outcomes, and ComplicationsАндрей ПетровBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- DR Pugud - Correlation Between CHD and DiabetesDokumen47 halamanDR Pugud - Correlation Between CHD and DiabetesKrishnaBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- 2009 CAQ Answers PDFDokumen80 halaman2009 CAQ Answers PDFAlex OprisanBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Vitamin EDokumen11 halamanVitamin EErvan Apsara BismakaBelum ada peringkat
- Adulthood & Geriatric PsychiatryDokumen13 halamanAdulthood & Geriatric PsychiatryPernel Jose Alam MicuboBelum ada peringkat
- Star Care Health Insurance PolicyDokumen20 halamanStar Care Health Insurance PolicyLuna DanielBelum ada peringkat
- Region 2 - Community-Based Services - September 2017Dokumen12 halamanRegion 2 - Community-Based Services - September 2017Jennifer BankerBelum ada peringkat
- Bahasa Inggris: Taking Vital Sign (Injection)Dokumen7 halamanBahasa Inggris: Taking Vital Sign (Injection)iyal09Belum ada peringkat
- Wart Removal and TreatmentDokumen6 halamanWart Removal and TreatmentwandaBelum ada peringkat
- Non Surgical Therapy For Anal Fissure (Review) - Cochrane LibraryDokumen118 halamanNon Surgical Therapy For Anal Fissure (Review) - Cochrane LibraryNicolás CopaniBelum ada peringkat
- BAUTISTA, DYANNE G. - Oncology Nursing Colorectal Cancer Case StudyDokumen16 halamanBAUTISTA, DYANNE G. - Oncology Nursing Colorectal Cancer Case StudyDyanne BautistaBelum ada peringkat
- Consort ChecklistDokumen2 halamanConsort ChecklistAyuAnatrieraBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)