Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- A-Plus Beyond Critical Shield A-Plus Beyond Early Critical Shield Brochure 8thDokumen21 halamanA-Plus Beyond Critical Shield A-Plus Beyond Early Critical Shield Brochure 8thNavin IndranBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- De Lima 20Dokumen14 halamanDe Lima 20Juhi VermaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Physical Assessment Sample1Dokumen6 halamanPhysical Assessment Sample1Allan Dela CruzBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Cystic Teraoma - CT DetectionDokumen5 halamanCystic Teraoma - CT DetectionagathapradanaBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Non Ulcerative Dyspepsia Secondary To Stress DisorderDokumen79 halamanNon Ulcerative Dyspepsia Secondary To Stress Disorderromeo rivera100% (1)
- Zamzam WaterDokumen6 halamanZamzam Wateranak amanahBelum ada peringkat
- Irfan Mir NotesDokumen199 halamanIrfan Mir NotesSwathi AnantulaBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Same Sex Adoption EvDokumen5 halamanSame Sex Adoption Evapi-292471795Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Vasculitis SyndromesDokumen56 halamanVasculitis SyndromesHengki Permana PutraBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Treatment For ESRDDokumen9 halamanTreatment For ESRDpunpen ngorsakun100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
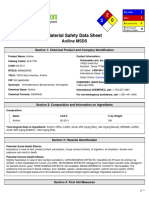
- Msds Aniline PDFDokumen6 halamanMsds Aniline PDFMika PelagioBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Handbook CarcinogenicDokumen279 halamanHandbook CarcinogenicNada Fitrieyatul HikmahBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Guide To Clinical Differential Diagnosis PDFDokumen41 halamanA Guide To Clinical Differential Diagnosis PDFNisa Nafiah OktavianiBelum ada peringkat
- Protein Folding Proposal (Huntingtin)Dokumen3 halamanProtein Folding Proposal (Huntingtin)yuyupyupchemBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Benefits Analysis Application Process FAX COVER LETTERDokumen10 halamanBenefits Analysis Application Process FAX COVER LETTERmdugan5026Belum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Complete Rates CGHSDokumen32 halamanComplete Rates CGHSAnkur MittalBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Chlamydia Power PointDokumen19 halamanChlamydia Power PointAnne McfarlandBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- 0529 Protocol Update 6.2.09 PDFDokumen57 halaman0529 Protocol Update 6.2.09 PDFTowhidulIslamBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Application of Radiotracer in MedicineDokumen17 halamanApplication of Radiotracer in MedicineUsama NazeerBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Self-Assessment Quiz: Introduction To Epidemiology Page 1-85Dokumen75 halamanSelf-Assessment Quiz: Introduction To Epidemiology Page 1-85Coy Nuñez100% (4)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- CCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormDokumen1 halamanCCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormMigori ArtBelum ada peringkat
- Resveratrol and Its Effects On Human Health and LongevityDokumen367 halamanResveratrol and Its Effects On Human Health and LongevityArnulfo Yu LanibaBelum ada peringkat
- Lets Talk About Health Fun Activities Games Oneonone Activities Pronuncia - 1996Dokumen1 halamanLets Talk About Health Fun Activities Games Oneonone Activities Pronuncia - 1996jadransko moreBelum ada peringkat
- Sdo PM QF Sgod SHN 001 Students Health Card ElementaryDokumen3 halamanSdo PM QF Sgod SHN 001 Students Health Card ElementaryShiela E. EladBelum ada peringkat
- Trends in Molecular Medicine - December 2013Dokumen51 halamanTrends in Molecular Medicine - December 2013Kevin SavouryBelum ada peringkat
- S&P Pharma Industry Overview - 11252010Dokumen49 halamanS&P Pharma Industry Overview - 11252010earajesh100% (1)
- Nutrition and Weight ManagementDokumen185 halamanNutrition and Weight ManagementKritika Taya100% (1)
- Material Safety Data Sheet: Phenolphthalein, IndicatorDokumen5 halamanMaterial Safety Data Sheet: Phenolphthalein, IndicatorYomi MedaBelum ada peringkat
- 1.D/D of Intraconal Mass 2.D/D of Leucocoria 3.U/S & CT Findings of RB 4.how Will You Manage That CaseDokumen15 halaman1.D/D of Intraconal Mass 2.D/D of Leucocoria 3.U/S & CT Findings of RB 4.how Will You Manage That CaseMuhammad SharjeelBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Advanced Special Subject 9.2Dokumen22 halamanAdvanced Special Subject 9.2Nguyen Ngoc Khoi NguyenBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)