Anda mungkin juga menyukai
- Night Final ProjectDokumen3 halamanNight Final ProjectLsm2139Belum ada peringkat
- Mock ABRSM Practical ExamDokumen2 halamanMock ABRSM Practical ExamLogan100% (2)
- WHO - Health Researchers GuideDokumen235 halamanWHO - Health Researchers Guidejonlim78Belum ada peringkat
- RUM NewDokumen53 halamanRUM NewbennyBelum ada peringkat
- Achieveing A DreamDokumen3 halamanAchieveing A Dreamvenera1108Belum ada peringkat
- S20054en PDFDokumen434 halamanS20054en PDFnuraji090689Belum ada peringkat
- WHO Advocates 12 Key Interventions To Promote More Rational UseDokumen4 halamanWHO Advocates 12 Key Interventions To Promote More Rational UseAsfa MarediaBelum ada peringkat
- The World Medicines Situation 2011 Traditional Medicines - Global Situation, Issues and ChallengesDokumen14 halamanThe World Medicines Situation 2011 Traditional Medicines - Global Situation, Issues and ChallengesBlogWatchBelum ada peringkat
- Rational Use of Medicines: Progress in Implementing The WHO Medicines StrategyDokumen7 halamanRational Use of Medicines: Progress in Implementing The WHO Medicines StrategyDoctor StrangeBelum ada peringkat
- RC53 09Dokumen5 halamanRC53 09gabriela_mariangela5929Belum ada peringkat
- Prevention and Containment of Antimicrobial Resistance: Sixty-Third Session Bangkok, Thailand 7-10 September 2010Dokumen17 halamanPrevention and Containment of Antimicrobial Resistance: Sixty-Third Session Bangkok, Thailand 7-10 September 2010gabriela_mariangela5929Belum ada peringkat
- Conceptual Litfor Research Lit ForlocDokumen13 halamanConceptual Litfor Research Lit ForlocMaria Angelika BughaoBelum ada peringkat
- Rational Drug UseDokumen18 halamanRational Drug UseSuresh ThanneruBelum ada peringkat
- Dic 4 51Dokumen4 halamanDic 4 51amritaryaaligarghBelum ada peringkat
- Pharmaceutical Development in Developing WorldDokumen28 halamanPharmaceutical Development in Developing WorldMay NguyenBelum ada peringkat
- Specs RlamfiltersDokumen8 halamanSpecs RlamfiltersananthBelum ada peringkat
- Intravenous Drug UseDokumen6 halamanIntravenous Drug Usemarionnasimiyu2001Belum ada peringkat
- Falsified Medicines and The Global Public's Health: InsightDokumen24 halamanFalsified Medicines and The Global Public's Health: InsightAndromeda KalapoyoBelum ada peringkat
- Progress in The Rational Use of Medicines: Report by The SecretariatDokumen4 halamanProgress in The Rational Use of Medicines: Report by The SecretariatUmu ZeynabBelum ada peringkat
- Ecec 03 00052Dokumen4 halamanEcec 03 00052Matiyas ZewdeBelum ada peringkat
- Essential DrugsDokumen20 halamanEssential DrugsReem 10Belum ada peringkat
- Research Report On Self-Medication in UgandaDokumen48 halamanResearch Report On Self-Medication in UgandaNev Ille80% (10)
- Irrational Use of DrugDokumen9 halamanIrrational Use of Drugsreedam100% (2)
- Lisa Forman Trade Rules and Human RightsDokumen21 halamanLisa Forman Trade Rules and Human RightsVictor Zamora Mesía100% (1)
- Multidrug-Resistant Tuberculosis (MDR-TB) Is Defined As TB That Is Resistant To BothDokumen4 halamanMultidrug-Resistant Tuberculosis (MDR-TB) Is Defined As TB That Is Resistant To Bothsanny_sundariBelum ada peringkat
- Chapter 1Dokumen48 halamanChapter 1placalus nimbusBelum ada peringkat
- REFERAT Anak TasiaDokumen15 halamanREFERAT Anak TasiaAnastasia PasaribuBelum ada peringkat
- Polypharmacy and Drug-Related Problems Among People Living With HIV-AIDS - A Single-Center Experience (#577802) - 735759Dokumen8 halamanPolypharmacy and Drug-Related Problems Among People Living With HIV-AIDS - A Single-Center Experience (#577802) - 735759LauraBelum ada peringkat
- The Pharmacist's Role in Preventing Antibiotic Resistance: Abstract and IntroductionDokumen5 halamanThe Pharmacist's Role in Preventing Antibiotic Resistance: Abstract and IntroductionDeginaraBelum ada peringkat
- Problems of Irrational Drug Use: Session GuideDokumen22 halamanProblems of Irrational Drug Use: Session Guidearyo aryoBelum ada peringkat
- WHO PanoramaDokumen16 halamanWHO PanoramaimsBelum ada peringkat
- Pharmacovigilance Ensuring The Safe Use of MedicinesDokumen18 halamanPharmacovigilance Ensuring The Safe Use of MedicinespopadrianionutzBelum ada peringkat
- 7 Rational PharmacotherapeuticsDokumen5 halaman7 Rational PharmacotherapeuticssistaBelum ada peringkat
- International Journal of Business and Management Invention (IJBMI)Dokumen8 halamanInternational Journal of Business and Management Invention (IJBMI)inventionjournalsBelum ada peringkat
- Healthcare Resources RephraseDokumen4 halamanHealthcare Resources RephraseMarium FatimaBelum ada peringkat
- Registration of Antimicrobials, Kenya, Uganda and United Republic of Tanzania, 2018Dokumen18 halamanRegistration of Antimicrobials, Kenya, Uganda and United Republic of Tanzania, 2018h3493061Belum ada peringkat
- Promoting Rational Use of Medicines: A Publication of The World Council of ChurchesDokumen32 halamanPromoting Rational Use of Medicines: A Publication of The World Council of ChurchesMarthaBelum ada peringkat
- Medicines in Health Systems Working Toward UHC: Presentation ScriptDokumen21 halamanMedicines in Health Systems Working Toward UHC: Presentation ScriptHananAhmedBelum ada peringkat
- PolypharmacyDokumen4 halamanPolypharmacyJeffrey Tan100% (1)
- ACMP BrNoteGenrl en Feb09Dokumen4 halamanACMP BrNoteGenrl en Feb09dangrandiBelum ada peringkat
- The Pharmacist - S Role in Preventing Antibiotic Resistance PDFDokumen8 halamanThe Pharmacist - S Role in Preventing Antibiotic Resistance PDFalfox2000Belum ada peringkat
- Assignment 1Dokumen3 halamanAssignment 1Alfie16Belum ada peringkat
- Rational Use of Drugs 10 BDokumen39 halamanRational Use of Drugs 10 BAnonymous DgPsK0oQ100% (1)
- Treatment of Medical, Psychiatric, and Substance-Use Comorbidities in People Infected With HIV Who Use DrugsDokumen21 halamanTreatment of Medical, Psychiatric, and Substance-Use Comorbidities in People Infected With HIV Who Use Drugsjuan_bacha_1Belum ada peringkat
- The Antibiotic Self-Medication Practices of Residents of Iloilo CityDokumen17 halamanThe Antibiotic Self-Medication Practices of Residents of Iloilo CityLALABelum ada peringkat
- Multidrug and Extensively Drug-Resistant TB (M/XDR-TB) : 2010 Global Report On Surveillance and ResponseDokumen71 halamanMultidrug and Extensively Drug-Resistant TB (M/XDR-TB) : 2010 Global Report On Surveillance and ResponseRachmad SanjayaBelum ada peringkat
- Dangers of Injections Overuse in Developing Countries With A High HIV/ AIDS Prevalence: A Review On HIV Risk Hazards, Traumatic Effects and Other Blood Borne InfectionsDokumen6 halamanDangers of Injections Overuse in Developing Countries With A High HIV/ AIDS Prevalence: A Review On HIV Risk Hazards, Traumatic Effects and Other Blood Borne InfectionsRizki Bagus MaulanaBelum ada peringkat
- Knowledge and Adherence To Antiretroviral Therapy Among Adult People Living With HIV/AIDS Treated in The Health Care Centers of The Association "Espoir Vie Togo" in Togo, West AfricaDokumen7 halamanKnowledge and Adherence To Antiretroviral Therapy Among Adult People Living With HIV/AIDS Treated in The Health Care Centers of The Association "Espoir Vie Togo" in Togo, West AfricanazargafarBelum ada peringkat
- Ch6 19rareDokumen4 halamanCh6 19rareArmin BiparvaBelum ada peringkat
- Antibiotic Use and Resistance in Emerging Economies: A Situation Analysis For Viet NamDokumen10 halamanAntibiotic Use and Resistance in Emerging Economies: A Situation Analysis For Viet NamKhánh HuyềnBelum ada peringkat
- The Treasure Called AntibioticsDokumen2 halamanThe Treasure Called AntibioticsBenamrane MarwaBelum ada peringkat
- Medicines Promotion: Assessing The Nature, Extent and Impact of RegulationDokumen38 halamanMedicines Promotion: Assessing The Nature, Extent and Impact of RegulationAsmitaBelum ada peringkat
- The Necessity of Overcoming The Menace and Dangers of Self Medication SEMINAR 2022Dokumen16 halamanThe Necessity of Overcoming The Menace and Dangers of Self Medication SEMINAR 2022ridwan sanusiBelum ada peringkat
- Pa Issue Brief FinalDokumen21 halamanPa Issue Brief FinalAsja AvdićBelum ada peringkat
- Self PDFDokumen5 halamanSelf PDFTommy Winahyu PuriBelum ada peringkat
- JIAPAC Editorial 2016 UNGASS On World Drug Program Pre Print 041416Dokumen6 halamanJIAPAC Editorial 2016 UNGASS On World Drug Program Pre Print 041416Rosa NovitaBelum ada peringkat
- Session 10 Essential Medicine SelectionDokumen23 halamanSession 10 Essential Medicine SelectionPhaimBelum ada peringkat
- The Basis For Self-Medication Interested ConsumersDokumen5 halamanThe Basis For Self-Medication Interested ConsumersRasco BiBelum ada peringkat
- Pharmaceutical Waste in The Environment: A Cultural PerspectiveDokumen6 halamanPharmaceutical Waste in The Environment: A Cultural PerspectiveTerrence Terry BhengoeBelum ada peringkat
- World Health Organization Patient SafetyDokumen4 halamanWorld Health Organization Patient SafetyMassLiveBelum ada peringkat
- S 6169 eDokumen98 halamanS 6169 eRizki M H IndrawanBelum ada peringkat
- Herbal medicine: Herbal Antibiotics ,The Ultimate Guide Guide to Healing Common AilmentsDari EverandHerbal medicine: Herbal Antibiotics ,The Ultimate Guide Guide to Healing Common AilmentsBelum ada peringkat
- Course Director Guide: Training Course On The Management of Severe MalnutritionDokumen28 halamanCourse Director Guide: Training Course On The Management of Severe MalnutritionkabambaBelum ada peringkat
- Part Three: Training Facilitators: 1. General Structure of The Facilitator Training SessionDokumen30 halamanPart Three: Training Facilitators: 1. General Structure of The Facilitator Training SessionkabambaBelum ada peringkat
- Clin Inst GuideDokumen45 halamanClin Inst GuidekabambaBelum ada peringkat
- Aea06 GPBrochureDokumen2 halamanAea06 GPBrochurekabambaBelum ada peringkat
- DiabetesDokumen118 halamanDiabeteskabambaBelum ada peringkat
- DHM Manual InWEntDokumen27 halamanDHM Manual InWEntkabambaBelum ada peringkat
- Clean Asceptic and Sterile TechniquesDokumen21 halamanClean Asceptic and Sterile TechniqueskabambaBelum ada peringkat
- Obstetrics Common Dilemmas-WFBuysDokumen34 halamanObstetrics Common Dilemmas-WFBuyskabambaBelum ada peringkat
- Topic 3: (Chapters From) Chapter 9: Logic of Hypothesis TestingDokumen2 halamanTopic 3: (Chapters From) Chapter 9: Logic of Hypothesis TestingkabambaBelum ada peringkat
- Basic Princinciples of Infection ControlDokumen46 halamanBasic Princinciples of Infection ControlkabambaBelum ada peringkat
- Closing The Gap Between Gen A RationsDokumen256 halamanClosing The Gap Between Gen A RationsCarolina Kramer100% (1)
- 07 CS NormalPostopEvalDokumen3 halaman07 CS NormalPostopEvalkabambaBelum ada peringkat
- Health Care Quality ImprovementDokumen188 halamanHealth Care Quality Improvementkabamba100% (2)
- Humanistic Training Techniques: The Use of Anatomic ModelsDokumen5 halamanHumanistic Training Techniques: The Use of Anatomic ModelskabambaBelum ada peringkat
- Case Study: Eclampsia: DirectionsDokumen1 halamanCase Study: Eclampsia: DirectionskabambaBelum ada peringkat
- Neda ProjectsDokumen23 halamanNeda Projectsminus25Belum ada peringkat
- Whitaker - Commodity Ecology Wheel (130 Version), Description, Biography, June 2019 W Prototype Link On First PageDokumen3 halamanWhitaker - Commodity Ecology Wheel (130 Version), Description, Biography, June 2019 W Prototype Link On First PagemwhitakerBelum ada peringkat
- Tips CAE Speaking TestDokumen5 halamanTips CAE Speaking TestYosoyJohnnyBravoBelum ada peringkat
- All Wiley-Blackwell JournalsDokumen454 halamanAll Wiley-Blackwell JournalsSeif EddineBelum ada peringkat
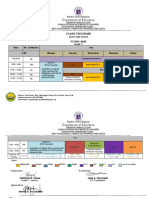
- Class Program Grade 7-10Dokumen9 halamanClass Program Grade 7-10jake felicianoBelum ada peringkat
- Example of Resume For CriminologyDokumen6 halamanExample of Resume For Criminologyaffguqiec100% (1)
- Essay Writing in ExamsDokumen4 halamanEssay Writing in ExamsKashif WaqasBelum ada peringkat
- Monthly College Budget: Year Income: Year Expenses: Year Cash FlowDokumen1 halamanMonthly College Budget: Year Income: Year Expenses: Year Cash FlowTagel MarkosBelum ada peringkat
- Ped 3138 Place Story - Gina Morphy-3Dokumen6 halamanPed 3138 Place Story - Gina Morphy-3api-252825989Belum ada peringkat
- Geriatria en MexicoDokumen7 halamanGeriatria en MexicoMarioGxBelum ada peringkat
- Digital Competency FrameworkDokumen15 halamanDigital Competency FrameworkNoah OkitoiBelum ada peringkat
- Connectives PDFDokumen2 halamanConnectives PDFDanijelaBelum ada peringkat
- Arjun Mishra TeachingDokumen2 halamanArjun Mishra TeachingArjun MishraBelum ada peringkat
- PressedDokumen198 halamanPressedThe DarkBelum ada peringkat
- Kontrolės Sąrašas (MIGRIS, UTPĮ 40.1.4 (1), Mėlynoji Kortelė, Išduoti LLG) (01) - USDokumen2 halamanKontrolės Sąrašas (MIGRIS, UTPĮ 40.1.4 (1), Mėlynoji Kortelė, Išduoti LLG) (01) - USYoussef AbdelkhalekBelum ada peringkat
- H1B Visa Interview QuestionsDokumen2 halamanH1B Visa Interview QuestionsRicky RicsBelum ada peringkat
- NEP 2020 Suggested ChangesDokumen21 halamanNEP 2020 Suggested ChangesAnuragBelum ada peringkat
- Culture UAEDokumen12 halamanCulture UAEanant_jain88114Belum ada peringkat
- Conflict Essay Lessons and Student PapersDokumen9 halamanConflict Essay Lessons and Student PapersKatharine Johnson100% (1)
- East Centralite 1916-1919Dokumen180 halamanEast Centralite 1916-1919Katherine SleykoBelum ada peringkat
- Midterm EvaluationDokumen3 halamanMidterm Evaluationapi-312642927Belum ada peringkat
- BI Y5 LP TS25 - Civic EducationDokumen2 halamanBI Y5 LP TS25 - Civic EducationThurga AB KrishenanBelum ada peringkat
- Apprenticeship+ AdevertisementDokumen9 halamanApprenticeship+ Adevertisementaltaf0987ssBelum ada peringkat
- LaserLyte's Trigger Tyme™ Laser Training PistolDokumen3 halamanLaserLyte's Trigger Tyme™ Laser Training PistolTwobirds Flying PublicationsBelum ada peringkat
- Listofe ReturnIntermediaries OperationalDokumen6 halamanListofe ReturnIntermediaries OperationalnaniBelum ada peringkat
- The Social Studies Curriculum:Retrospect and ProspectDokumen38 halamanThe Social Studies Curriculum:Retrospect and ProspectNathalie DeduqueBelum ada peringkat
- NCBTS Volume 1 Teachingprof Socdime FS 219 273Dokumen112 halamanNCBTS Volume 1 Teachingprof Socdime FS 219 273justin may tuyorBelum ada peringkat
- DLP # 43 Summative TestDokumen5 halamanDLP # 43 Summative TestRitz Anton Lim100% (1)