Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Dorothy Johnson PosterDokumen1 halamanDorothy Johnson Posterapi-519455077Belum ada peringkat
- Theology of The BodyDokumen2 halamanTheology of The BodyKim JuanBelum ada peringkat
- ObamaDeception SupplementalBookletDokumen34 halamanObamaDeception SupplementalBookletAccurateHistorian100% (4)
- Texas Medicaid and CHIP Provider FAQsDokumen4 halamanTexas Medicaid and CHIP Provider FAQsangelina smithBelum ada peringkat
- Reason J. Human ErrorDokumen3 halamanReason J. Human ErrorDanielaGarciaBelum ada peringkat
- Poverty Is General Scarcity or The State of One Who Lacks A Certain Amount of Material Possessions or MoneyDokumen41 halamanPoverty Is General Scarcity or The State of One Who Lacks A Certain Amount of Material Possessions or MoneyChristian Cañon GenterolaBelum ada peringkat
- Alwyn Naicker - Research Proposal Assignment 2 PDFDokumen15 halamanAlwyn Naicker - Research Proposal Assignment 2 PDFAlwyn NaickerBelum ada peringkat
- ShowfileDokumen19 halamanShowfileiyalazhaguBelum ada peringkat
- Table 5.1-2 Minnesota Multiphasic Personality Inventory Validity and Clinical Scales ValidityDokumen4 halamanTable 5.1-2 Minnesota Multiphasic Personality Inventory Validity and Clinical Scales ValidityReisya GinaBelum ada peringkat
- Freedom From DistractibilityDokumen4 halamanFreedom From DistractibilityΚων/να ΠαπBelum ada peringkat
- Aira Noreen Leyva - Resume ReviewDokumen2 halamanAira Noreen Leyva - Resume Reviewapi-447475293Belum ada peringkat
- WHO Guidelines Hand Hygiene in Health CareDokumen270 halamanWHO Guidelines Hand Hygiene in Health CareÐr Salma100% (1)
- Complicated GrievingDokumen117 halamanComplicated GrievingEra Galuh100% (1)
- Microbiology-Disinfectants Lab ReportDokumen2 halamanMicrobiology-Disinfectants Lab Reportsaraebo25% (4)
- Sinif Ingilizce 8. Unite Calisma Kagidi Test Etkinlik Worksheet FITNESS by Murat DukkanciDokumen13 halamanSinif Ingilizce 8. Unite Calisma Kagidi Test Etkinlik Worksheet FITNESS by Murat DukkanciElif yurtsevenBelum ada peringkat
- BCG - The Future of Jobs in The Era of AI - 2021 - NeiDokumen40 halamanBCG - The Future of Jobs in The Era of AI - 2021 - NeiHevertom FischerBelum ada peringkat
- Chemistry, Manufacturing and ControlDokumen11 halamanChemistry, Manufacturing and ControlHk HkBelum ada peringkat
- Body Parts Lesson PlanDokumen3 halamanBody Parts Lesson Planapi-372758719Belum ada peringkat
- HgedgergtDokumen84 halamanHgedgergtWRGWSRBelum ada peringkat
- NCP Acute Pain Related To Tissue Ischemia As Manifested by Changes in Level of Consciousness PDFDokumen3 halamanNCP Acute Pain Related To Tissue Ischemia As Manifested by Changes in Level of Consciousness PDFOGNTVBelum ada peringkat
- Big Drugs!!Dokumen2.145 halamanBig Drugs!!Solomon Seth SallforsBelum ada peringkat
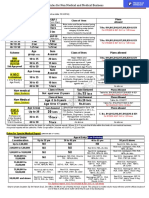
- Rules For Non Medical BusinessDokumen1 halamanRules For Non Medical BusinessAbhijit AminpurBelum ada peringkat
- A Guide To Safety Committee Meeting Tech3Dokumen5 halamanA Guide To Safety Committee Meeting Tech3vsrslm100% (1)
- Dengue Virus: A Vexatious "RED" FeverDokumen6 halamanDengue Virus: A Vexatious "RED" FeverDr. Hussain NaqviBelum ada peringkat
- EnSURE Touch - F&BDokumen6 halamanEnSURE Touch - F&BfaradillafattaBelum ada peringkat
- Tranexamic Acid MouthwashDokumen1 halamanTranexamic Acid MouthwashTalal MazharBelum ada peringkat
- Hospital Income Benefit Plan HIBDokumen2 halamanHospital Income Benefit Plan HIBIngrid SastrilloBelum ada peringkat
- Fall Prevention: How Can Older Adults Prevent Falls?Dokumen4 halamanFall Prevention: How Can Older Adults Prevent Falls?Amalina ZahariBelum ada peringkat
- NammaKPSC - February 2020Dokumen138 halamanNammaKPSC - February 2020anandawarBelum ada peringkat
- Postpartum Hemorrhage: Prevention and Treatment: Table 1Dokumen10 halamanPostpartum Hemorrhage: Prevention and Treatment: Table 1erikafebriyanarBelum ada peringkat