Anda mungkin juga menyukai
- Diagno SIS Planni NG Intervention Rationale Evaluati ONDokumen3 halamanDiagno SIS Planni NG Intervention Rationale Evaluati ONAnn Nicole G. NeriBelum ada peringkat
- Nursing and End-of-Life CareDokumen26 halamanNursing and End-of-Life CareShafiq Ur RahmanBelum ada peringkat
- I and I Module Infectious DisordersDokumen23 halamanI and I Module Infectious DisordersCaitlynBelum ada peringkat
- I and I MODULE INFECTIOUS DISORDERSDokumen23 halamanI and I MODULE INFECTIOUS DISORDERSJeffrey GazmenBelum ada peringkat
- Learning Feedback DiaryDokumen2 halamanLearning Feedback DiaryReyna Mee AhiyasBelum ada peringkat
- Infectious and Inflammatory DisordersDokumen84 halamanInfectious and Inflammatory DisordersMariel OracoyBelum ada peringkat
- MDRTB Case StudyDokumen35 halamanMDRTB Case StudyFejlean Angelica AntineoBelum ada peringkat
- Guillain Barre SyndromeDokumen21 halamanGuillain Barre Syndromebasinang_jangilBelum ada peringkat
- Clinical Management Protocol PDFDokumen7 halamanClinical Management Protocol PDFAJEET KUMAR PANDEYBelum ada peringkat
- ReportDokumen4 halamanReportKyle DapulagBelum ada peringkat
- Infections in ICUDokumen7 halamanInfections in ICUNikolay ToméBelum ada peringkat
- Control of Diarrheal Diseases (CDD) : ObjectivesDokumen39 halamanControl of Diarrheal Diseases (CDD) : ObjectivesKatrina CaveBelum ada peringkat
- Natural History of DiseaseDokumen26 halamanNatural History of Diseaseadinda mouzasBelum ada peringkat
- Module 12: Infection Control in Health Care Settings: Image Courtesy Of: World Lung FoundationDokumen37 halamanModule 12: Infection Control in Health Care Settings: Image Courtesy Of: World Lung FoundationAniruddhaBelum ada peringkat
- Nursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationDokumen3 halamanNursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationPaul Cubacub100% (1)
- 5 Nursing Management TBDokumen2 halaman5 Nursing Management TBًBelum ada peringkat
- Learning Material RLE NCM 112Dokumen5 halamanLearning Material RLE NCM 112shiro the catBelum ada peringkat
- Caring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyDokumen34 halamanCaring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyRubinaBelum ada peringkat
- Presentation 1Dokumen20 halamanPresentation 1Akshita JainBelum ada peringkat
- BPOC in Medicina PrimaraDokumen3 halamanBPOC in Medicina PrimaraAlina GheBelum ada peringkat
- Prophylactic Measures: Sneha Ganesh 2 Yr MbbsDokumen25 halamanProphylactic Measures: Sneha Ganesh 2 Yr MbbsSneha GaneshBelum ada peringkat
- Use of Antibiotics 2017Dokumen17 halamanUse of Antibiotics 2017bernard.triciaBelum ada peringkat
- 312 Respi Scenario ReviewerDokumen13 halaman312 Respi Scenario Reviewer11 - JEMELYN LOTERTEBelum ada peringkat
- Swine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiaDokumen19 halamanSwine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiagirismgBelum ada peringkat
- Care of Critically Ill Patient:: Johny Wilbert, M.SC (N)Dokumen40 halamanCare of Critically Ill Patient:: Johny Wilbert, M.SC (N)Nancy SinghBelum ada peringkat
- UntitledDokumen7 halamanUntitledAkash HalsanaBelum ada peringkat
- Pulmonary TBDokumen13 halamanPulmonary TBAmanda ScarletBelum ada peringkat
- Fresh H1N1 Guidelines 1 - 1-18Dokumen15 halamanFresh H1N1 Guidelines 1 - 1-18Shahid IqbalBelum ada peringkat
- Ncar (Sr. Nerlyn)Dokumen9 halamanNcar (Sr. Nerlyn)nerlynBelum ada peringkat
- Tuberculosis: Angeles University FoundationDokumen10 halamanTuberculosis: Angeles University FoundationBob Joyce Dela PeñaBelum ada peringkat
- Influenza Bhasa InggrisDokumen11 halamanInfluenza Bhasa InggrisandiniBelum ada peringkat
- Nursing Management 1Dokumen8 halamanNursing Management 1Melai AvilaBelum ada peringkat
- Lung Cancer (Nursing Care)Dokumen5 halamanLung Cancer (Nursing Care)heiyuBelum ada peringkat
- Rational Use of AntibioticsDokumen85 halamanRational Use of AntibioticsAHMAD MAHIR BIN CHE RAHMATBelum ada peringkat
- Prophylactics of PneumoniaDokumen31 halamanProphylactics of PneumoniaJoisy AloorBelum ada peringkat
- NCP CysticDokumen2 halamanNCP Cysticapi-30271420250% (2)
- PNEUMONIADokumen24 halamanPNEUMONIAwheeyycoldandhot55Belum ada peringkat
- Supporting Patient and Family Processes: Heart Failure and Pulmonary EdemaDokumen6 halamanSupporting Patient and Family Processes: Heart Failure and Pulmonary EdemaAnonymous oEinbIijNnBelum ada peringkat
- Group 1 Case Study Chapter 24Dokumen10 halamanGroup 1 Case Study Chapter 24Doneva Lyn MedinaBelum ada peringkat
- NSG MGT Asthma (Autosaved)Dokumen14 halamanNSG MGT Asthma (Autosaved)sarikaBelum ada peringkat
- Dengue FeverDokumen1 halamanDengue Feverapi-266482250Belum ada peringkat
- Detailed Lesson Plan in Health 8Dokumen7 halamanDetailed Lesson Plan in Health 8trisha abad73% (11)
- Principles of Disease Control and PreventionDokumen13 halamanPrinciples of Disease Control and PreventionAYO NELSON0% (1)
- Prevention of Infection: Infectious Diseases Global HealthDokumen12 halamanPrevention of Infection: Infectious Diseases Global HealthsaravananBelum ada peringkat
- Compendium Adult 2015 Press Rev3Dokumen2 halamanCompendium Adult 2015 Press Rev3Yudha Ardi NBelum ada peringkat
- Nursing Diagnosis Impaired Gas ExchangeDokumen7 halamanNursing Diagnosis Impaired Gas ExchangeZycon Rodney Ae'zecquel Gachallan50% (2)
- Inp Cu 7 CopdDokumen26 halamanInp Cu 7 CopdMichelle Gliselle Guinto MallareBelum ada peringkat
- CD Part 2 - Communicable Diseases With Pics (1) ConDokumen239 halamanCD Part 2 - Communicable Diseases With Pics (1) ConMackoi SalamanesBelum ada peringkat
- ACTIVITIESDokumen6 halamanACTIVITIESArvin PenalosaBelum ada peringkat
- Inp Midterms MergedDokumen67 halamanInp Midterms MergedMichelle Gliselle Guinto MallareBelum ada peringkat
- PneumoniaDokumen71 halamanPneumoniafrancis00090100% (1)
- TB Nursing CareplanDokumen14 halamanTB Nursing CareplanEstherThompson100% (1)
- Presentation 1Dokumen10 halamanPresentation 1Abdulla AshourBelum ada peringkat
- Edit NG Drug StudyDokumen35 halamanEdit NG Drug StudyAlleinad BarracasBelum ada peringkat
- Chapter Five Summary of Findings, Conclusion and RecommendationsDokumen5 halamanChapter Five Summary of Findings, Conclusion and RecommendationsKojo AduBelum ada peringkat
- World's Deadliest Disease and Remains A Major Public Health Problem in The PhilippinesDokumen17 halamanWorld's Deadliest Disease and Remains A Major Public Health Problem in The Philippineslorella_abejuelaBelum ada peringkat
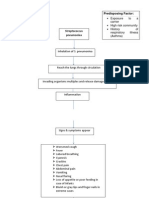
- Precipitating Factors: Predisposing FactorDokumen4 halamanPrecipitating Factors: Predisposing FactorRoxanne Ganayo ClaverBelum ada peringkat
- PneumoniaDokumen3 halamanPneumoniaErwin SmithBelum ada peringkat
- SocializationDokumen42 halamanSocializationLag Lag AlbercaBelum ada peringkat
- Physical Changes That Occurs During AdolescenceDokumen1 halamanPhysical Changes That Occurs During AdolescenceLag Lag AlbercaBelum ada peringkat
- Havighurst'S Developmental Tasks During The Life SpanDokumen2 halamanHavighurst'S Developmental Tasks During The Life SpanLag Lag AlbercaBelum ada peringkat
- Powerpoint Presentation Prepared By: Terri Petkau, Mohawk CollegeDokumen29 halamanPowerpoint Presentation Prepared By: Terri Petkau, Mohawk CollegeLag Lag AlbercaBelum ada peringkat
- Prepared By: (A4) Nurul Syazana Binti Zainuddin Amanina Zahirah Binti Zulkifle Siti Hajar Binti HassanDokumen13 halamanPrepared By: (A4) Nurul Syazana Binti Zainuddin Amanina Zahirah Binti Zulkifle Siti Hajar Binti HassanLag Lag AlbercaBelum ada peringkat
- Selection and Organization of Content DalimbangDokumen18 halamanSelection and Organization of Content DalimbangLag Lag Alberca100% (1)
- Emotional PatternDokumen5 halamanEmotional PatternLag Lag Alberca100% (1)
- Core Competencies in NursingDokumen11 halamanCore Competencies in NursingBadz Tan100% (1)
- ASPERGILLOMADokumen6 halamanASPERGILLOMALag Lag AlbercaBelum ada peringkat
- Nephrotic Syndrome FinalDokumen11 halamanNephrotic Syndrome FinalLag Lag AlbercaBelum ada peringkat
- Drug StudyDokumen33 halamanDrug StudyLag Lag AlbercaBelum ada peringkat
- Benign Prostatic HyperplasiaDokumen5 halamanBenign Prostatic HyperplasiaLag Lag AlbercaBelum ada peringkat
- G 10 ICT WorkSheetc 2.2 English MDokumen8 halamanG 10 ICT WorkSheetc 2.2 English MMohamaad SihatthBelum ada peringkat
- Drugs and Tinnitus - Neil Bauman PHD - April '09Dokumen2 halamanDrugs and Tinnitus - Neil Bauman PHD - April '09DownTheTheRabbitHole108Belum ada peringkat
- 0900-9914 I1 201012 PDFDokumen132 halaman0900-9914 I1 201012 PDFIvan Arjona50% (2)
- Aspire 7535 ManualDokumen220 halamanAspire 7535 ManualinklabsBelum ada peringkat
- Reading Week 13Dokumen6 halamanReading Week 13Quy PhanBelum ada peringkat
- Patel, Anita - Super Indian Snack and Street Food Recipes PDFDokumen117 halamanPatel, Anita - Super Indian Snack and Street Food Recipes PDFBella ImèneBelum ada peringkat
- Bravo Petroleum ProfileDokumen8 halamanBravo Petroleum ProfileJacob Thom ZiwahwaBelum ada peringkat
- Unit 2 - CT2Dokumen45 halamanUnit 2 - CT2Jagrit DusejaBelum ada peringkat
- DuranDuran OrdinaryWorldDokumen1 halamanDuranDuran OrdinaryWorldEduardo LuzBelum ada peringkat
- Gunny PasteDokumen2 halamanGunny PastejpesBelum ada peringkat
- Metal-Tek Electric Contact Cleaner Spray - TDS (2021)Dokumen1 halamanMetal-Tek Electric Contact Cleaner Spray - TDS (2021)metal-tek asteBelum ada peringkat
- Allegheny Power Planning CriteriaDokumen19 halamanAllegheny Power Planning Criteriaksdp1Belum ada peringkat
- Genmega G2500Dokumen103 halamanGenmega G2500tchindaforentBelum ada peringkat
- Festivals of IndiaDokumen51 halamanFestivals of IndiaDhatchayani RamkumarBelum ada peringkat
- 4864.21 - Optics System 2Dokumen39 halaman4864.21 - Optics System 2Edgar Jose Aponte MartinezBelum ada peringkat
- GTE LAB MANUAL Ver 4 - 1Dokumen135 halamanGTE LAB MANUAL Ver 4 - 1akhilaBelum ada peringkat
- Gas AbsorptionDokumen93 halamanGas AbsorptionArgie Adduru73% (11)
- Colegio de San Gabriel Arcangel of Caloocan, IncDokumen7 halamanColegio de San Gabriel Arcangel of Caloocan, IncKIRITO SALINASBelum ada peringkat
- Traina 250Wp PDFDokumen2 halamanTraina 250Wp PDFSherifImamBelum ada peringkat
- Stephane Moses The Angel of History Rosenzweig Benjamin Scholem PDFDokumen196 halamanStephane Moses The Angel of History Rosenzweig Benjamin Scholem PDFlivehuman100% (3)
- The Tenth House in AstrologyDokumen6 halamanThe Tenth House in AstrologytratakBelum ada peringkat
- Method Statement For Boom Barrier Installation (Rev00) ELV2Dokumen38 halamanMethod Statement For Boom Barrier Installation (Rev00) ELV2balajiBelum ada peringkat
- The Rheological Properties of Ketchup As A Function of Different Hydrocolloids and TemperatureDokumen8 halamanThe Rheological Properties of Ketchup As A Function of Different Hydrocolloids and TemperatureVicente WiethBelum ada peringkat
- Ecological Fire MGMT Guidelines V5Dokumen40 halamanEcological Fire MGMT Guidelines V5MeBelum ada peringkat
- Introduction To Mass Transfer - Part 1Dokumen39 halamanIntroduction To Mass Transfer - Part 1Biniyam haile100% (1)
- HP 300s+ Scientific Calculator: Sophisticated Design Ideal For Math and Science StudentsDokumen3 halamanHP 300s+ Scientific Calculator: Sophisticated Design Ideal For Math and Science StudentsgemaBelum ada peringkat
- Dimensional Stability After MoldingDokumen14 halamanDimensional Stability After MoldingpgovindaiahBelum ada peringkat
- Ovonic Unified Memory OR Phase Change MemoryDokumen37 halamanOvonic Unified Memory OR Phase Change Memoryrockstar_69Belum ada peringkat
- R0221120 - Salsabilla Cindy Pratama - Daily ActivityDokumen15 halamanR0221120 - Salsabilla Cindy Pratama - Daily Activitysalsabilla cindy pratamaBelum ada peringkat
- SOAL UAS Kelas 12Dokumen8 halamanSOAL UAS Kelas 12amirBelum ada peringkat