Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Kidney HistogenesisDokumen9 halamanKidney HistogenesisKshitija KasturiBelum ada peringkat
- Grade 8 - 4thquarter - BiotechDokumen11 halamanGrade 8 - 4thquarter - BiotechChrista dana ReyesBelum ada peringkat
- Management of Deep Carious LesionsDokumen5 halamanManagement of Deep Carious LesionsEmeka V. ObiBelum ada peringkat
- Hester-Biosciences Karvy 010915 PDFDokumen17 halamanHester-Biosciences Karvy 010915 PDFmannimanojBelum ada peringkat
- Anticoagulant Activity of Paragis Pudadera Et. AlDokumen35 halamanAnticoagulant Activity of Paragis Pudadera Et. Alvanessa piraanBelum ada peringkat
- Challis, Debbie The Archaeology of Race The Eugenic Ideas of FrancisDokumen217 halamanChallis, Debbie The Archaeology of Race The Eugenic Ideas of FrancisSonicoBelum ada peringkat
- IMN1207 McGillActiveProtocolsDokumen11 halamanIMN1207 McGillActiveProtocolsapi-3714923Belum ada peringkat
- DNA - The Double Helix: Chromosomes Are Composed of Genes. A Gene Is A Segment of DNA ThatDokumen4 halamanDNA - The Double Helix: Chromosomes Are Composed of Genes. A Gene Is A Segment of DNA Thatapi-310760045Belum ada peringkat
- Hemostasis, Surgical Bleeding and TransfusionDokumen10 halamanHemostasis, Surgical Bleeding and TransfusionCarl Earvin L. FavoritoBelum ada peringkat
- BISC202 PracticeEXM 1Dokumen7 halamanBISC202 PracticeEXM 1Layomi Dele-DareBelum ada peringkat
- Diagnostic Criteria For The Behavioral Variant FTDDokumen5 halamanDiagnostic Criteria For The Behavioral Variant FTDMusleh AlgarniBelum ada peringkat
- RT-5 Unit 2 QPDokumen7 halamanRT-5 Unit 2 QPbiotecnika_testBelum ada peringkat
- Cystic Fibrosis Foundation: Richmond's Finest 2017Dokumen4 halamanCystic Fibrosis Foundation: Richmond's Finest 2017Richmond MagazineBelum ada peringkat
- Male Reproductive Physiology - UpToDate - 2020Dokumen18 halamanMale Reproductive Physiology - UpToDate - 2020Karaca AzizBelum ada peringkat
- Sample Pages of MBBS Decode (MGR University)Dokumen20 halamanSample Pages of MBBS Decode (MGR University)vkBelum ada peringkat
- Comparative Circulatory SystemDokumen15 halamanComparative Circulatory SystemSmartcool SoBelum ada peringkat
- Adaptive Immunity: Shimelis Teshome (BSC MLS)Dokumen31 halamanAdaptive Immunity: Shimelis Teshome (BSC MLS)Shimelis Teshome AyalnehBelum ada peringkat
- Gene TherapyDokumen29 halamanGene TherapypriyankaBelum ada peringkat
- Clinical Practice Guideline For Management For Rehabilitation of Lower Limb AmputationDokumen55 halamanClinical Practice Guideline For Management For Rehabilitation of Lower Limb Amputationburtyx100% (1)
- Antigen Presenting CellDokumen26 halamanAntigen Presenting CellSurja DasBelum ada peringkat
- Biology of Domestic Animals PDFDokumen371 halamanBiology of Domestic Animals PDFfeketerigo67% (3)
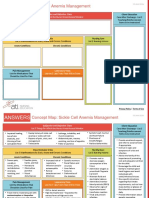
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDokumen2 halamanNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- CMV Quant PCRDokumen82 halamanCMV Quant PCRyousrazeidan1979Belum ada peringkat
- Chapter 18. Mood StabilizersDokumen12 halamanChapter 18. Mood StabilizersAlfen PranataBelum ada peringkat
- The Bull's Eye - May 2011Dokumen13 halamanThe Bull's Eye - May 2011dbhsbullseyeBelum ada peringkat
- Cambridge IGCSE: Biology 0610/22Dokumen16 halamanCambridge IGCSE: Biology 0610/22Aisha YousifBelum ada peringkat
- Antibacterials 2018 PDFDokumen203 halamanAntibacterials 2018 PDFfdfdfdfBelum ada peringkat
- Endocrine System Notes - NCERT BasedDokumen8 halamanEndocrine System Notes - NCERT Basedpallab mukherjeeBelum ada peringkat
- Teratology: Handbook ofDokumen478 halamanTeratology: Handbook ofmaria5basBelum ada peringkat
- Pediatrics in Review 2012 McCavit 195 206Dokumen14 halamanPediatrics in Review 2012 McCavit 195 206cindyBelum ada peringkat