Anda mungkin juga menyukai
- Reporting Suspected Adverse Drug ReactionsDokumen2 halamanReporting Suspected Adverse Drug ReactionsWajeeha HassanBelum ada peringkat
- Report of Suspected Adverse Drug Reactions: It's Easy To Report Online: Mhra - Gov.uk/yellowcard or Via The AppDokumen2 halamanReport of Suspected Adverse Drug Reactions: It's Easy To Report Online: Mhra - Gov.uk/yellowcard or Via The AppGeorgia KavakopoulouBelum ada peringkat
- Report of Suspected Adverse Reaction To Medicines or VaccinesDokumen2 halamanReport of Suspected Adverse Reaction To Medicines or VaccinesSidhaSaada PatelBelum ada peringkat
- Reporting Form for Suspected ASU Drug ReactionsDokumen2 halamanReporting Form for Suspected ASU Drug ReactionsSachin JadonBelum ada peringkat
- What To Include in Your Yellow Card of An Adverse Drug ReactionDokumen3 halamanWhat To Include in Your Yellow Card of An Adverse Drug Reactionrhimineecat71Belum ada peringkat
- Program Name Medication Application Type StatusDokumen6 halamanProgram Name Medication Application Type StatusLiatisha McneilBelum ada peringkat
- Lecture 1 IntroductionDokumen8 halamanLecture 1 IntroductionManWol JangBelum ada peringkat
- Northyx, Tapazole (Methimazole) Dosing, Indications, Interactions, Adverse Effects, and MoreDokumen2 halamanNorthyx, Tapazole (Methimazole) Dosing, Indications, Interactions, Adverse Effects, and MoreDewiAryani11Belum ada peringkat
- Therapeutic Use Exemption (Tue) : 1. Player InformationDokumen4 halamanTherapeutic Use Exemption (Tue) : 1. Player InformationSeremet ValentinaBelum ada peringkat
- WISCONSIN INFORMED CONSENT FOR OPIOID ANTAGONIST MEDICATIONDokumen3 halamanWISCONSIN INFORMED CONSENT FOR OPIOID ANTAGONIST MEDICATIONdnutter012576Belum ada peringkat
- Pat Ms IIDokumen18 halamanPat Ms IIapi-339980385Belum ada peringkat
- Inpatient Notes Drafted by N.Yieko: Nicholas Yieko (COMPANY NAME) (Company Address)Dokumen6 halamanInpatient Notes Drafted by N.Yieko: Nicholas Yieko (COMPANY NAME) (Company Address)nicholasBelum ada peringkat
- Medication Error Reporting FormDokumen3 halamanMedication Error Reporting FormRani WulandariBelum ada peringkat
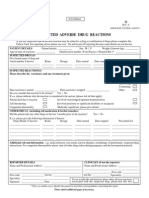
- Suspected Adverse Drug Reaction Reporting Form: CdscoDokumen2 halamanSuspected Adverse Drug Reaction Reporting Form: CdscoNaveen Kumar G TBelum ada peringkat
- Adverse Drug ReactionsDokumen54 halamanAdverse Drug ReactionsAprilVivienCu100% (2)
- BENSAL KASUKA__HOSPITAL AND COMMUNITY PHARMACY PRACTICES QUESTIONSDokumen40 halamanBENSAL KASUKA__HOSPITAL AND COMMUNITY PHARMACY PRACTICES QUESTIONSHussein KadagaraBelum ada peringkat
- Patient Education on PrednisoneDokumen6 halamanPatient Education on PrednisoneLenie DayanghirangBelum ada peringkat
- Suspected Adverse Drug Reactions: in ConfidenceDokumen1 halamanSuspected Adverse Drug Reactions: in ConfidenceSujith KuttanBelum ada peringkat
- 10 TH Conf Poly PharmacyDokumen5 halaman10 TH Conf Poly Pharmacytr14niBelum ada peringkat
- Pharmacist Role in Healthcare System - New ZealandDokumen44 halamanPharmacist Role in Healthcare System - New ZealandFelicia AngelineBelum ada peringkat
- Drug (Glucophage)Dokumen2 halamanDrug (Glucophage)mchaudry7Belum ada peringkat
- Pharmacovigilance - An Overview: Dr. Sukanta Sen MD, DNB, DM (Clin Pharmacology)Dokumen31 halamanPharmacovigilance - An Overview: Dr. Sukanta Sen MD, DNB, DM (Clin Pharmacology)FranchescaAmoréBrodithe100% (1)
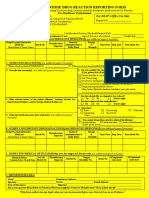
- DRAP New Suspected Adverse Reaction Reporting Form For Health Care Professionals PDFDokumen3 halamanDRAP New Suspected Adverse Reaction Reporting Form For Health Care Professionals PDFShakil Khan100% (1)
- Pat FundamentalsDokumen16 halamanPat Fundamentalsapi-339980385Belum ada peringkat
- Pharmacology Group 3Dokumen9 halamanPharmacology Group 3wiyadiBelum ada peringkat
- Black Triangle SchemeDokumen4 halamanBlack Triangle SchemeSusan RosaBelum ada peringkat
- Adverse: Drug Reaction ReportingDokumen2 halamanAdverse: Drug Reaction ReportingSofie DyahBelum ada peringkat
- History and Objectives of Postmarketing Drug SurveillanceDokumen14 halamanHistory and Objectives of Postmarketing Drug SurveillanceSohit Gupta100% (1)
- Adverse Drug Reactions ExplainedDokumen71 halamanAdverse Drug Reactions ExplainedVaibhav ThoratBelum ada peringkat
- NCSBN Practice Knowledge Network Call: Off-Label Drug Use 1/10/2013Dokumen23 halamanNCSBN Practice Knowledge Network Call: Off-Label Drug Use 1/10/2013Ari NurfikriBelum ada peringkat
- Analysis of The Strength and Weakness of The Different Methods For Detection of Adverse Drug ReactionsDokumen11 halamanAnalysis of The Strength and Weakness of The Different Methods For Detection of Adverse Drug ReactionsRohitBelum ada peringkat
- Pat Semester 1Dokumen17 halamanPat Semester 1api-300946501Belum ada peringkat
- How To Fill ADR Reporitng Form and Causality AssessmentDokumen38 halamanHow To Fill ADR Reporitng Form and Causality AssessmentVishal AryaBelum ada peringkat
- InstructionToFill ADRformDokumen4 halamanInstructionToFill ADRformJahnavi PutrevuBelum ada peringkat
- National Pharmacovigilance Centre, Botswana: Started StoppedDokumen3 halamanNational Pharmacovigilance Centre, Botswana: Started StoppedMikelAgberoBelum ada peringkat
- Primolut N en PiDokumen12 halamanPrimolut N en Piakinbileje2002Belum ada peringkat
- Patient Medication ReviewDokumen4 halamanPatient Medication ReviewRoxcee88Belum ada peringkat
- PharmacovigilanceDokumen43 halamanPharmacovigilanceTanoy SahaBelum ada peringkat
- GUIDELINES FOR PRESCRIPTIONDokumen8 halamanGUIDELINES FOR PRESCRIPTIONsequeira123Belum ada peringkat
- MTM Pre-Seminar Exercise Materials - 2Dokumen17 halamanMTM Pre-Seminar Exercise Materials - 2Enoch Ko4% (23)
- Drug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver DiseaseDokumen20 halamanDrug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver Diseaseal ghiffari muhammad rayhan100% (1)
- Safe Medication PrinciplesDokumen39 halamanSafe Medication PrinciplesAnastasia Yovita SariBelum ada peringkat
- Medican Marijuana Request FormDokumen3 halamanMedican Marijuana Request FormLouis C. HochmanBelum ada peringkat
- Drug Template - Preparation Phase of Learning Using The Big 3Dokumen1 halamanDrug Template - Preparation Phase of Learning Using The Big 3sunshine10chemBelum ada peringkat
- Appointment Details: NHS ConfidentialDokumen2 halamanAppointment Details: NHS ConfidentialYash Vardhan DeoraBelum ada peringkat
- Vol 14 No 2a Vortioxetine For Depression Jan 2016Dokumen2 halamanVol 14 No 2a Vortioxetine For Depression Jan 2016John SmithBelum ada peringkat
- Adr Form 10Dokumen3 halamanAdr Form 10doctor uroosaBelum ada peringkat
- ADR FormDokumen2 halamanADR Formapi-3810976Belum ada peringkat
- Fenoterol Inhalation SolutionDokumen2 halamanFenoterol Inhalation SolutionkurniawanBelum ada peringkat
- Bulletin June2011Dokumen6 halamanBulletin June2011Rema Panickar SugunanBelum ada peringkat
- MTM ToolsDokumen8 halamanMTM ToolsEbrahimDawudBelum ada peringkat
- Medication Errors: Causes, Types & PreventionDokumen4 halamanMedication Errors: Causes, Types & PreventionJoyce TanBelum ada peringkat
- Pharmacovigilance: The Science of Monitoring Drug SafetyDokumen29 halamanPharmacovigilance: The Science of Monitoring Drug SafetyMaurizio Sessa100% (1)
- Adverse Event ReportingDokumen2 halamanAdverse Event ReportingSanjay NavaleBelum ada peringkat
- Rational Prescribing Guide for Safe MedicationDokumen6 halamanRational Prescribing Guide for Safe MedicationJohannes WelchBelum ada peringkat
- Cefoxitin and Ketorolac Edited!!Dokumen3 halamanCefoxitin and Ketorolac Edited!!Bryan Cruz VisarraBelum ada peringkat
- Monitoring Efek Samping Obat (MESO)Dokumen25 halamanMonitoring Efek Samping Obat (MESO)Nienies NurikaBelum ada peringkat
- S C111910 PrescribingDrugs Council Nov192010Dokumen7 halamanS C111910 PrescribingDrugs Council Nov192010Ilham Maulana HerdiansyahBelum ada peringkat
- Irish Pharmacist May 09Dokumen44 halamanIrish Pharmacist May 09John MaguireBelum ada peringkat
- Practical Prescribing for Musculoskeletal Practitioners 2/eDari EverandPractical Prescribing for Musculoskeletal Practitioners 2/eBelum ada peringkat
- Brushing Force of Manual and Sonic Toothbrushes Affects Dental Hard Tissue AbrasionDokumen25 halamanBrushing Force of Manual and Sonic Toothbrushes Affects Dental Hard Tissue AbrasionLeonardo AlcotaBelum ada peringkat
- ARSENAL Hospital OvalleDokumen23 halamanARSENAL Hospital OvalleLeonardo AlcotaBelum ada peringkat
- Canales Cloro Acoplados GABADokumen6 halamanCanales Cloro Acoplados GABALeonardo AlcotaBelum ada peringkat
- SD ArticleDokumen16 halamanSD ArticleLeonardo AlcotaBelum ada peringkat
- Crown LengtheningDokumen12 halamanCrown LengtheningKesavaa Vasuthaven100% (1)
- Critical Care Updates: CPR Guidelines and In-Hospital Cardiac Arrest PreventionDokumen23 halamanCritical Care Updates: CPR Guidelines and In-Hospital Cardiac Arrest PreventionkhayanBelum ada peringkat
- Williams, Sue Death of A Doctor How The Medical Profession Turned On One of Their Own PDFDokumen324 halamanWilliams, Sue Death of A Doctor How The Medical Profession Turned On One of Their Own PDFmahendranBelum ada peringkat
- ICD 10 in IndiaDokumen59 halamanICD 10 in IndiaAseem Sharma50% (2)
- Sage Char-Lee Letter of Recomendation 2Dokumen1 halamanSage Char-Lee Letter of Recomendation 2api-510197139Belum ada peringkat
- Acl Rehab ProtocolDokumen37 halamanAcl Rehab ProtocolkhaldoonBelum ada peringkat
- Ethics in Pharmacy Practice: Under Supervision Of: DR Noha M SalehDokumen24 halamanEthics in Pharmacy Practice: Under Supervision Of: DR Noha M SalehEyad NabilBelum ada peringkat
- Making AppointmentDokumen6 halamanMaking AppointmentNabila PramestiBelum ada peringkat
- SCOTTISH HOSPITAL PHARMACY PLACEMENT GUIDEDokumen29 halamanSCOTTISH HOSPITAL PHARMACY PLACEMENT GUIDEKostas KoutsodimosBelum ada peringkat
- Hospital: Building AttributesDokumen7 halamanHospital: Building AttributesPatricia ParinasBelum ada peringkat
- Pre-Grad Learning PlanDokumen2 halamanPre-Grad Learning Planapi-283968269Belum ada peringkat
- Blood Transfusio ChecklistDokumen6 halamanBlood Transfusio ChecklistJLea OchiaBelum ada peringkat
- EC Medical Reimbursement Application Form 1Dokumen2 halamanEC Medical Reimbursement Application Form 1GaryBelum ada peringkat
- The Stony Brook Press - Volume 30, Issue 11Dokumen44 halamanThe Stony Brook Press - Volume 30, Issue 11The Stony Brook PressBelum ada peringkat
- Nurse job application letterDokumen1 halamanNurse job application letterGiegie NuescaBelum ada peringkat
- MediCard Philippines Naga - List of PediatriciansDokumen4 halamanMediCard Philippines Naga - List of PediatriciansJared HaberBelum ada peringkat
- Maintenance of Supplies and EquipmentsDokumen11 halamanMaintenance of Supplies and EquipmentsCheranmadevi Padavettan100% (1)
- Hand SanitizerDokumen2 halamanHand SanitizerPrince WamiqBelum ada peringkat
- Porter 5 Force ModelDokumen41 halamanPorter 5 Force ModelSatish J. Makwana0% (1)
- Self Reflective JournalDokumen3 halamanSelf Reflective Journalapi-448502475Belum ada peringkat
- SSM Application SummaryDokumen61 halamanSSM Application SummarySeptaPratamaAptBelum ada peringkat
- Lecture For Community Health CareDokumen7 halamanLecture For Community Health CareagbrittainBelum ada peringkat
- High Eficency Particular Air Filter: Multizone DopairDokumen2 halamanHigh Eficency Particular Air Filter: Multizone DopairarmanBelum ada peringkat
- Reviewer in ICTM111Dokumen4 halamanReviewer in ICTM111Angelie Marian100% (1)
- HealtheMed Launch Press Release 091620 FinalDokumen2 halamanHealtheMed Launch Press Release 091620 FinalFluenceMediaBelum ada peringkat
- DR - Gowing AdvisoryDokumen2 halamanDR - Gowing AdvisorykaylekayprBelum ada peringkat
- Morse Fall ScaleDokumen8 halamanMorse Fall ScaleENTIN DARTINIBelum ada peringkat
- Đề thi chọn hsg quốc gia 2006 bảng BDokumen10 halamanĐề thi chọn hsg quốc gia 2006 bảng BChi MinhBelum ada peringkat
- Pharmacy Service VA Design Guide: Final DraftDokumen75 halamanPharmacy Service VA Design Guide: Final DraftAhmad Gamal Elden MAhanyBelum ada peringkat
- DoD Ortho-Pod-Chiro-Sports Med Clinic Space CriteriaDokumen47 halamanDoD Ortho-Pod-Chiro-Sports Med Clinic Space CriteriaSiraj HaiderBelum ada peringkat