Anda mungkin juga menyukai
- 03mb5 17 PDFDokumen3 halaman03mb5 17 PDFKhusnah KhauliyaBelum ada peringkat
- 5 Senior ExercisesDokumen3 halaman5 Senior Exercisestamaki55Belum ada peringkat
- Lumbar Assessment Form 2017Dokumen2 halamanLumbar Assessment Form 2017nsboyadzhievBelum ada peringkat
- Acl CaseDokumen8 halamanAcl CaseLidia DebbyBelum ada peringkat
- Physiotherapy Advice After Your Kidney TransplantDokumen8 halamanPhysiotherapy Advice After Your Kidney TransplantAlexander ScottBelum ada peringkat
- Pediatric Physiotherapy Assessment Aidaaaaa 2Dokumen15 halamanPediatric Physiotherapy Assessment Aidaaaaa 2Khaled M.A. AlqedraBelum ada peringkat
- Bells Palsy Physio PDFDokumen71 halamanBells Palsy Physio PDFडा. सत्यदेव त्यागी आर्यBelum ada peringkat
- Physiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeDokumen9 halamanPhysiotherapy For Stroke Patients - Physiotherapy Remedies For Victims of StrokeHumaira RahmanBelum ada peringkat
- APA 7th Edition Template Student VersionDokumen14 halamanAPA 7th Edition Template Student VersionAndrei ArtiedaBelum ada peringkat
- Physical Therapy Management of Congenital Muscular.2Dokumen47 halamanPhysical Therapy Management of Congenital Muscular.2Katherine Valeska Sánchez MuñozBelum ada peringkat
- 215 PDFDokumen7 halaman215 PDFlewamBelum ada peringkat
- Rotator Cuff TendinopathyDokumen7 halamanRotator Cuff TendinopathyMarcus Dos SantosBelum ada peringkat
- Manual TherapyDokumen16 halamanManual TherapylecturioBelum ada peringkat
- Cadera Espástica en Parálisis Cerebral Tabla GMFCSDokumen2 halamanCadera Espástica en Parálisis Cerebral Tabla GMFCSElsa Ivon Perez Flores100% (1)
- Pusher Syndrome A Frequent But Little-Known Disturbance of Body Orientation PerceptionDokumen11 halamanPusher Syndrome A Frequent But Little-Known Disturbance of Body Orientation PerceptionKlgo Alex AyalaBelum ada peringkat
- Kinetic Control Cap1Dokumen17 halamanKinetic Control Cap1Yennifer Serna MoncadaBelum ada peringkat
- Effects of Maitland Mobilization and Mul PDFDokumen6 halamanEffects of Maitland Mobilization and Mul PDFKuroha Hagane KunBelum ada peringkat
- Extremitas FormDokumen2 halamanExtremitas FormAbdur RasyidBelum ada peringkat
- Scapular-Stabilization Exercises - Early-Intervention PrescriptionDokumen6 halamanScapular-Stabilization Exercises - Early-Intervention PrescriptionJohnnySnow100% (1)
- A Clinical Tool For Office Assessment of Lumbar Spine Stabilization Endurance PDFDokumen7 halamanA Clinical Tool For Office Assessment of Lumbar Spine Stabilization Endurance PDFNicolas BavarescoBelum ada peringkat
- Cools. Scapular Mechanics and RehabilitationDokumen9 halamanCools. Scapular Mechanics and RehabilitationWalter PelaezBelum ada peringkat
- MMT (Manual Muscle Testing)Dokumen18 halamanMMT (Manual Muscle Testing)Estu MahendraBelum ada peringkat
- Therapeutic Exercise 1 IntroductionDokumen30 halamanTherapeutic Exercise 1 IntroductionMyrgen TingsonBelum ada peringkat
- Proprioceptive Neuromuscular Facilitation (PNF)Dokumen76 halamanProprioceptive Neuromuscular Facilitation (PNF)Hasan KhawaldehBelum ada peringkat
- Appendix: Motor Control Training Intervention ManualDokumen32 halamanAppendix: Motor Control Training Intervention Manualgonchodiaz1703Belum ada peringkat
- ICUDokumen12 halamanICUNabilahBelum ada peringkat
- Understanding Spinal Segmental Sensitization As A New Concept of Pain and Employ Its Treatment StrategiesDokumen3 halamanUnderstanding Spinal Segmental Sensitization As A New Concept of Pain and Employ Its Treatment Strategiesheaven6938Belum ada peringkat
- Effects of Physioball and Conventional Floor Exercises On Early Phase Adaptations in Back and Abdominal Core Stability and Balance in Women 2003Dokumen5 halamanEffects of Physioball and Conventional Floor Exercises On Early Phase Adaptations in Back and Abdominal Core Stability and Balance in Women 2003rdkelsallBelum ada peringkat
- Lumbar Herniation Case StudyDokumen1 halamanLumbar Herniation Case Studyapi-238652699Belum ada peringkat
- Therapeutic Effectiveness of Instrument-Assisted SoftDokumen11 halamanTherapeutic Effectiveness of Instrument-Assisted SoftDra. Gabriela FerreiraBelum ada peringkat
- Functional Reach TestDokumen3 halamanFunctional Reach TestMarcelo Fabian Alvarado GijonBelum ada peringkat
- Neck Disability IndexDokumen2 halamanNeck Disability IndexDhimas Agung PrayogaBelum ada peringkat
- Bad Ragaz Ring Method Gamper Lambeck Chapter 4 Comp Aq TH (2010)Dokumen29 halamanBad Ragaz Ring Method Gamper Lambeck Chapter 4 Comp Aq TH (2010)Blajiu BeatriceBelum ada peringkat
- Physical Therapy Clinical Management.9 PDFDokumen24 halamanPhysical Therapy Clinical Management.9 PDFClaudia MicuBelum ada peringkat
- Neurological Physiotherapy Evaluation FormDokumen14 halamanNeurological Physiotherapy Evaluation FormHawi Natalie Tundang100% (1)
- Antenatal and Postnatal PPT PDFDokumen15 halamanAntenatal and Postnatal PPT PDFNikita -0251 EBelum ada peringkat
- 2012 Mirror Therapy For Improving Motor Function After StrokeDokumen68 halaman2012 Mirror Therapy For Improving Motor Function After StrokeMarcelo Ortiz Valenzuela100% (1)
- 10 Meter Walk Test ManguziDokumen1 halaman10 Meter Walk Test ManguziDavid SugiartoBelum ada peringkat
- Tug Test-A PDFDokumen1 halamanTug Test-A PDFalqurina norizkaBelum ada peringkat
- 3 - Shoulder ScaptionDokumen4 halaman3 - Shoulder ScaptionRafi BhattiBelum ada peringkat
- Assignment of Neurology (Repaired) .Docx - 1494344936467Dokumen24 halamanAssignment of Neurology (Repaired) .Docx - 1494344936467Amrit Preet KaurBelum ada peringkat
- McKenzie CONCEPT AnilDokumen12 halamanMcKenzie CONCEPT AnilSOUMYADEEP BHUINYABelum ada peringkat
- Brunstorm'sDokumen19 halamanBrunstorm'sHARSH 23 (Jalu)Belum ada peringkat
- Passive Scapular Adduction TestDokumen15 halamanPassive Scapular Adduction Testapi-468597987Belum ada peringkat
- Brunnstorm ApproachDokumen33 halamanBrunnstorm ApproachFareeha KausarBelum ada peringkat
- KneeDokumen2 halamanKneedrkmsk100% (1)
- Consenso de MunichDokumen10 halamanConsenso de MunichBartholomew AllenBelum ada peringkat
- PNFpresentationDokumen32 halamanPNFpresentationNarkeesh ArumugamBelum ada peringkat
- Brunnstrom ApproachDokumen33 halamanBrunnstrom ApproachAISHWARYA SWAMINATHANBelum ada peringkat
- Closed Kinetic Chain Exercises-2013Dokumen2 halamanClosed Kinetic Chain Exercises-2013inrmpt77Belum ada peringkat
- Adult Physiatric History and ExaminationDokumen11 halamanAdult Physiatric History and Examinationsylschebe22gmailBelum ada peringkat
- Hip Fracture BinderDokumen60 halamanHip Fracture BinderMiaBelum ada peringkat
- Physiotherapy Treatment of Shoulder Pain - REHABILITATION PRINCIPLES. Today S Topics. Rehabilitation of Rotator Cuff TendinopathyDokumen32 halamanPhysiotherapy Treatment of Shoulder Pain - REHABILITATION PRINCIPLES. Today S Topics. Rehabilitation of Rotator Cuff TendinopathyWalter PelaezBelum ada peringkat
- Effect of Maitland Spinal Mobilization Therapy Versus Conventional Therapy in Lumbar Spondylosis With RadiculopathyDokumen8 halamanEffect of Maitland Spinal Mobilization Therapy Versus Conventional Therapy in Lumbar Spondylosis With RadiculopathyjuancaBelum ada peringkat
- Therapeutic Exercise (I) : Theory and PracticeDokumen155 halamanTherapeutic Exercise (I) : Theory and PracticeAbdulrhman MohamedBelum ada peringkat
- Roods ApproachDokumen33 halamanRoods ApproachCedricFernandez100% (1)
- Joint Mobilizations PDFDokumen1 halamanJoint Mobilizations PDFErik TellezBelum ada peringkat
- Handout Carb Counting 508cDokumen38 halamanHandout Carb Counting 508cPeter ZachBelum ada peringkat
- SEC01Dokumen8 halamanSEC01Peter ZachBelum ada peringkat
- Nutrient TimingDokumen20 halamanNutrient TimingPeter ZachBelum ada peringkat
- Carbon Footprint SpreadsheetDokumen34 halamanCarbon Footprint SpreadsheetPeter ZachBelum ada peringkat
- Syllabus - F, A B 1Dokumen37 halamanSyllabus - F, A B 1Peter ZachBelum ada peringkat
- Samsung Galaxy Tab 8.9 LTEDokumen112 halamanSamsung Galaxy Tab 8.9 LTEPeter ZachBelum ada peringkat
- 10 Keys To Successful TradingDokumen22 halaman10 Keys To Successful TradingManojkumar NairBelum ada peringkat
- Event Processing On The WebDokumen53 halamanEvent Processing On The WebPeter ZachBelum ada peringkat
- Marketing Plan SampleDokumen100 halamanMarketing Plan SamplePeter ZachBelum ada peringkat
- An Introduction To Event ProcessingDokumen20 halamanAn Introduction To Event ProcessingPeter ZachBelum ada peringkat
- Event Driven Architecture OverviewDokumen9 halamanEvent Driven Architecture OverviewPeter ZachBelum ada peringkat
- RC Cola Marketing PlanDokumen4 halamanRC Cola Marketing PlanJeff JosephBelum ada peringkat
- Marketing Plan SampleDokumen100 halamanMarketing Plan SamplePeter ZachBelum ada peringkat
- Example of A Marketing PlanDokumen41 halamanExample of A Marketing PlanLizi GrigorescuBelum ada peringkat
- Samsung Galaxy Tab 8.9 LTEDokumen112 halamanSamsung Galaxy Tab 8.9 LTEPeter ZachBelum ada peringkat
- Example of A Marketing PlanDokumen41 halamanExample of A Marketing PlanLizi GrigorescuBelum ada peringkat
- SEC01Dokumen8 halamanSEC01Peter ZachBelum ada peringkat
- RC Cola Marketing PlanDokumen4 halamanRC Cola Marketing PlanJeff JosephBelum ada peringkat
- Syllabus - F, A B 1Dokumen37 halamanSyllabus - F, A B 1Peter ZachBelum ada peringkat
- Bike Security at The University of WaterlooDokumen39 halamanBike Security at The University of WaterlooPeter ZachBelum ada peringkat
- CS 246 Object-Oriented Software DevelopmentDokumen220 halamanCS 246 Object-Oriented Software DevelopmentPeter ZachBelum ada peringkat
- SEC01Dokumen8 halamanSEC01Peter ZachBelum ada peringkat
- Woodies Cci Patterns and Terminology by Jim O'ConnellDokumen28 halamanWoodies Cci Patterns and Terminology by Jim O'ConnellAnonymous W7lVR9qs25Belum ada peringkat
- Bulletin July 2010Dokumen8 halamanBulletin July 2010Peter ZachBelum ada peringkat
- Anatomy and Pathophysiology of ProstrateDokumen44 halamanAnatomy and Pathophysiology of Prostraterajan kumar100% (3)
- Dr. Osama Mahmoud (Endocrinology)Dokumen253 halamanDr. Osama Mahmoud (Endocrinology)Mohammad Abd-AlhafezBelum ada peringkat
- HirudinomorphaDokumen3 halamanHirudinomorphaDave RapaconBelum ada peringkat
- Science Reviewer For Science Quiz Elementary: MatterDokumen30 halamanScience Reviewer For Science Quiz Elementary: MatterIan BelgaBelum ada peringkat
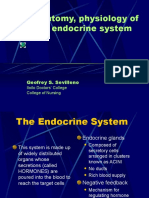
- Anatomy, Physiology of The Endocrine System: Geofrey S. SevillenoDokumen55 halamanAnatomy, Physiology of The Endocrine System: Geofrey S. Sevillenocoral jade cuaBelum ada peringkat
- OrchiectomyDokumen35 halamanOrchiectomyYosa Angga OktamaBelum ada peringkat
- Triangles of The NeckDokumen204 halamanTriangles of The Necknevmerka100% (3)
- Exam 3 Term 6 PDFDokumen3 halamanExam 3 Term 6 PDFThomas Santiago Torres CastroBelum ada peringkat
- اسايمنت البيدوDokumen2 halamanاسايمنت البيدوTasneem AbdBelum ada peringkat
- The Digestive System Graphic OrganiserDokumen1 halamanThe Digestive System Graphic Organiserapi-350307578100% (1)
- Physiology Chapter 30 Renal Regulation of PotassiumDokumen32 halamanPhysiology Chapter 30 Renal Regulation of PotassiumDaniel AdamsBelum ada peringkat
- MMRDokumen84 halamanMMRKelly YeowBelum ada peringkat
- Anatomy of Esophagus and StomachDokumen65 halamanAnatomy of Esophagus and Stomachmackiecc100% (2)
- The Cardiovascular System: The Heart: Essentials of Anatomy & PhysiologyDokumen23 halamanThe Cardiovascular System: The Heart: Essentials of Anatomy & PhysiologyJonalynCollodChewacheoBelum ada peringkat
- DETAILED LESSON PLAN IN SCIENCE5 Loida EmanoDokumen7 halamanDETAILED LESSON PLAN IN SCIENCE5 Loida EmanoVergiel Abellano88% (16)
- Immediate Physiological Changes in New BornDokumen7 halamanImmediate Physiological Changes in New BornLahunWanniangBelum ada peringkat
- Biochemical Changes During PregnancyDokumen15 halamanBiochemical Changes During Pregnancyz100% (1)
- ICD 10 Codes For Dental Practice: L PracticesDokumen9 halamanICD 10 Codes For Dental Practice: L PracticesAji HerlambangBelum ada peringkat
- Perineal Care: Figure 16.2, Giving Peri Care To FemalesDokumen2 halamanPerineal Care: Figure 16.2, Giving Peri Care To FemalesJurnalyn JupliBelum ada peringkat
- Class II Deep BiteDokumen12 halamanClass II Deep BitehabeebBelum ada peringkat
- Varicocele - Case StudyDokumen3 halamanVaricocele - Case StudyDanz AlsolBelum ada peringkat
- Golden 8 PDFDokumen23 halamanGolden 8 PDFcristi vBelum ada peringkat
- The Digestive SystemDokumen38 halamanThe Digestive SystemrabiaBelum ada peringkat
- Heart PhysiologyDokumen36 halamanHeart PhysiologyFrida Neila RahmatikaBelum ada peringkat
- RBI Script 12Dokumen4 halamanRBI Script 12Mary-Ann SanchezBelum ada peringkat
- Cure Your Migraines The Natural WayDokumen220 halamanCure Your Migraines The Natural WayAggie E KrolBelum ada peringkat
- GRADE 10 QUIZ EndocrineDokumen3 halamanGRADE 10 QUIZ EndocrineShielo Marie CabañeroBelum ada peringkat
- Pex 04 01Dokumen8 halamanPex 04 01Grace UrbanoBelum ada peringkat
- Heart AnatomyDokumen29 halamanHeart AnatomyKinga AndrasBelum ada peringkat
- Forensic DNA Analysis: DNA Is The Genetic MaterialDokumen71 halamanForensic DNA Analysis: DNA Is The Genetic MaterialumashankarbaghelBelum ada peringkat
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 4 dari 5 bintang4/5 (3)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincDari EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincPenilaian: 3.5 dari 5 bintang3.5/5 (137)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDari EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerDari EverandGut: the new and revised Sunday Times bestsellerPenilaian: 4 dari 5 bintang4/5 (392)
- Dark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseDari EverandDark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniversePenilaian: 3.5 dari 5 bintang3.5/5 (69)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsDari EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsPenilaian: 4.5 dari 5 bintang4.5/5 (6)
- The Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceDari EverandThe Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RacePenilaian: 4.5 dari 5 bintang4.5/5 (516)
- Masterminds: Genius, DNA, and the Quest to Rewrite LifeDari EverandMasterminds: Genius, DNA, and the Quest to Rewrite LifeBelum ada peringkat
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessDari EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessBelum ada peringkat
- Tales from Both Sides of the Brain: A Life in NeuroscienceDari EverandTales from Both Sides of the Brain: A Life in NeurosciencePenilaian: 3 dari 5 bintang3/5 (18)
- All That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesDari EverandAll That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesPenilaian: 4.5 dari 5 bintang4.5/5 (397)
- The Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionDari EverandThe Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionPenilaian: 4 dari 5 bintang4/5 (812)
- Undeniable: How Biology Confirms Our Intuition That Life Is DesignedDari EverandUndeniable: How Biology Confirms Our Intuition That Life Is DesignedPenilaian: 4 dari 5 bintang4/5 (11)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Dari EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Penilaian: 4 dari 5 bintang4/5 (378)
- 10% Human: How Your Body's Microbes Hold the Key to Health and HappinessDari Everand10% Human: How Your Body's Microbes Hold the Key to Health and HappinessPenilaian: 4 dari 5 bintang4/5 (33)
- Fast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperDari EverandFast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperPenilaian: 4.5 dari 5 bintang4.5/5 (15)
- Water: The Epic Struggle for Wealth, Power, and CivilizationDari EverandWater: The Epic Struggle for Wealth, Power, and CivilizationPenilaian: 3.5 dari 5 bintang3.5/5 (37)
- The Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorDari EverandThe Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorBelum ada peringkat
- The Rise and Fall of the Dinosaurs: A New History of a Lost WorldDari EverandThe Rise and Fall of the Dinosaurs: A New History of a Lost WorldPenilaian: 4 dari 5 bintang4/5 (595)
- Who's in Charge?: Free Will and the Science of the BrainDari EverandWho's in Charge?: Free Will and the Science of the BrainPenilaian: 4 dari 5 bintang4/5 (65)
- Good Without God: What a Billion Nonreligious People Do BelieveDari EverandGood Without God: What a Billion Nonreligious People Do BelievePenilaian: 4 dari 5 bintang4/5 (66)
- Seven and a Half Lessons About the BrainDari EverandSeven and a Half Lessons About the BrainPenilaian: 4 dari 5 bintang4/5 (109)
- Human: The Science Behind What Makes Your Brain UniqueDari EverandHuman: The Science Behind What Makes Your Brain UniquePenilaian: 3.5 dari 5 bintang3.5/5 (38)